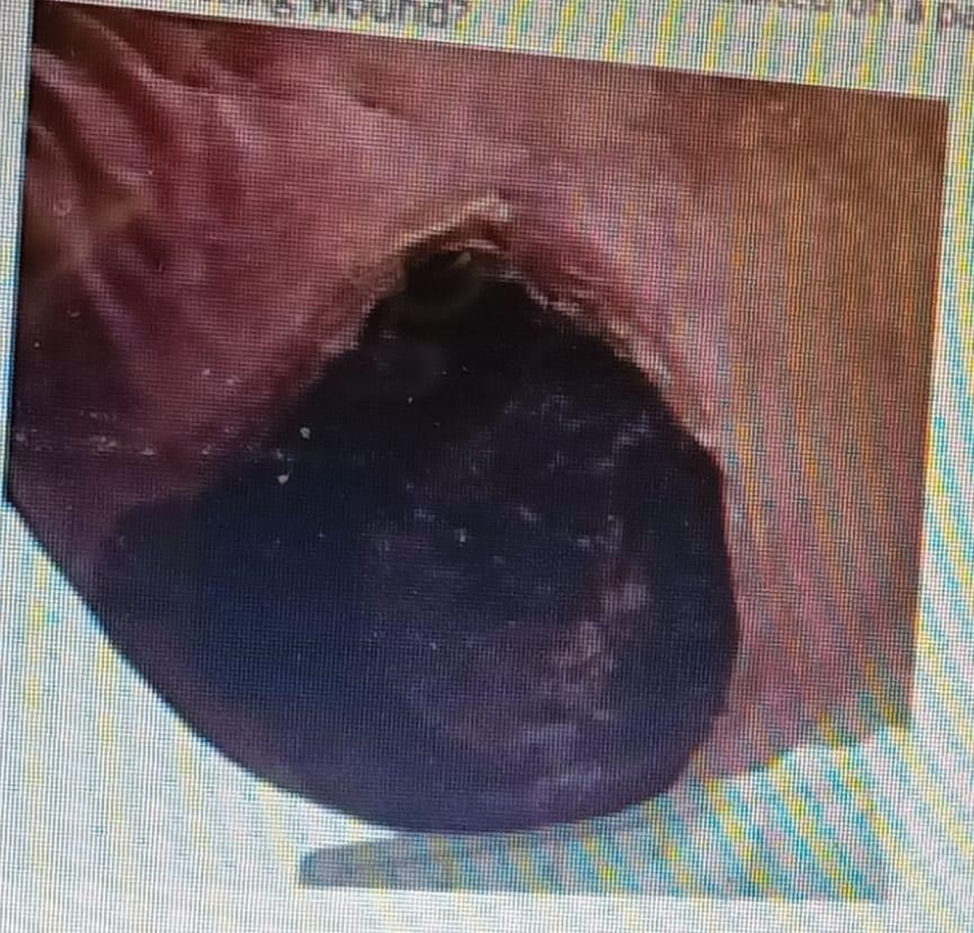
A wound care nurse has been consulted on a patient with multiple pressure wounds. The nurse comes across this heal wound. How should she document the following wound?
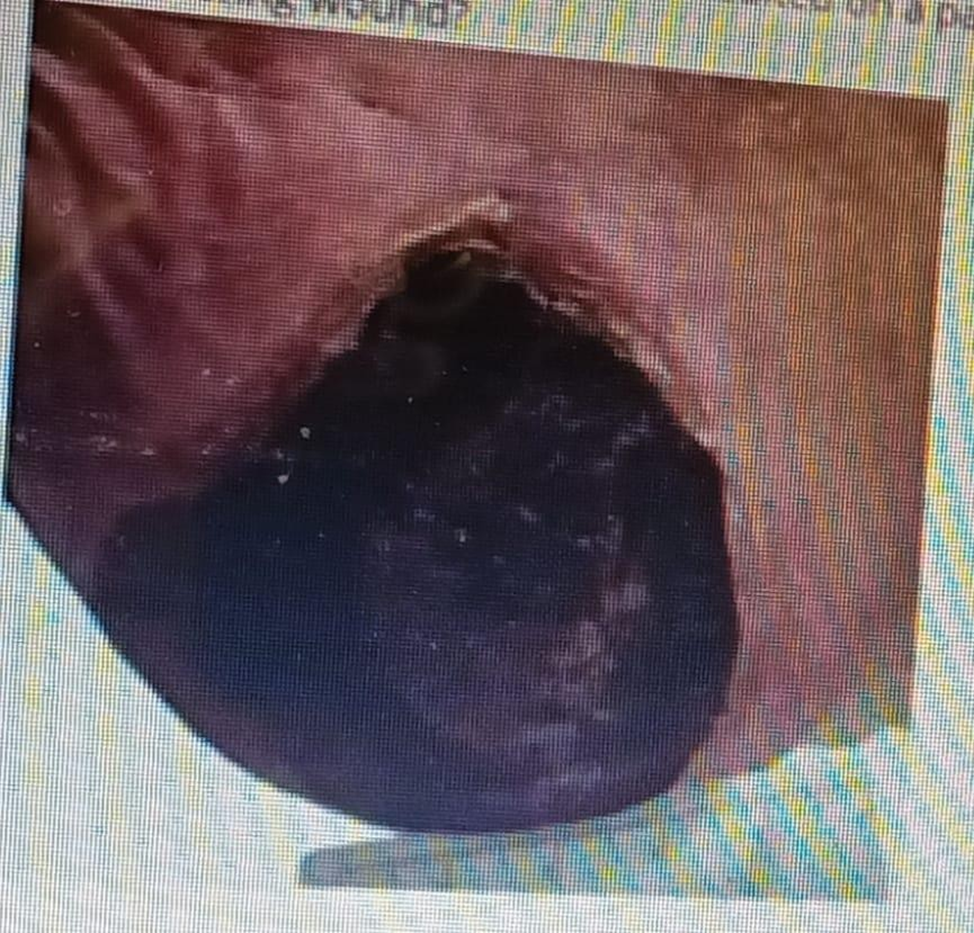
Unstageable Ulcer
Stage II Pressure Ulcer
Stage IV Pressure Ulcer
Stage III Pressure Ulcer
The Correct Answer is A
Choice A rationale: An unstageable ulcer is covered with slough or eschar, making it difficult to determine the depth of tissue involvement. The presence of eschar prevents accurate staging of the wound.
Choice B rationale: Stage II pressure ulcers involve partial-thickness skin loss, typically presenting as a shallow open ulcer with a red-pink wound bed.
Choice C rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed bone, tendon, or muscle, which is not described in this scenario.
Choice D rationale: Stage III pressure ulcers involve full-thickness tissue loss without exposed bone, tendon, or muscle, but the presence of eschar makes accurate staging challenging.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A rationale: The stool test for occult blood is not primarily designed to detect bacteria.
Choice B rationale: Parasites are not typically detected through a stool test for occult blood.
Choice C rationale: Steatorrhea refers to the presence of excess fat in the stool and is not the primary focus of a stool test for occult blood.
Choice D rationale: The purpose of the stool test for occult blood is to check for the presence of blood in the stool, which may not be visible to the naked eye. This can be an indicator of gastrointestinal bleeding.
Correct Answer is A
Explanation
Choice A rationale: An unstageable ulcer is covered with slough or eschar, making it difficult to determine the depth of tissue involvement. The presence of eschar prevents accurate staging of the wound.
Choice B rationale: Stage II pressure ulcers involve partial-thickness skin loss, typically presenting as a shallow open ulcer with a red-pink wound bed.
Choice C rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed bone, tendon, or muscle, which is not described in this scenario.
Choice D rationale: Stage III pressure ulcers involve full-thickness tissue loss without exposed bone, tendon, or muscle, but the presence of eschar makes accurate staging challenging.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today