A nursing diagnosis of "Risk for Deficient Fluid Volume" related to excessive fluid loss, secondary to diarrhea and vomiting was implemented for a home health client who began with these symptoms 5 days ago. A goal was set that the client's symptoms would be eliminated within 48 hours. The client is being seen after a week and has had no diarrhea or vomiting for the past 5 days. What should the nurse do?
Document that the potential problem is being prevented from recurring.
Document that the problem has been resolved and the goal has been met.
Assume that whatever the cause was, the symptoms may return, but the goal was met.
Keep the problem on the care plan in case the symptoms return.
The Correct Answer is B
The nursing diagnosis was "Risk for Deficient Fluid Volume" related to excessive fluid loss, secondary to diarrhea and vomiting. The goal was set that the client's symptoms would be eliminated within 48 hours. The client is being seen after a week and has had no diarrhea or vomiting for the past 5 days, indicating that the problem has been resolved. Therefore, the nurse should document that the problem has been resolved and the goal has been met.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
When selecting interventions for a care plan, the nurse should consider several principles. One important principle is that actions should address the underlying cause (etiology) of the nursing diagnosis. By addressing the root cause of the problem, interventions can be more effective in achieving the desired outcomes. There is not necessarily one "best" intervention for each goal or outcome, as different clients may have different needs and respond differently to interventions. Interventions can include both "doing" actions and monitoring, and both independent and collaborative interventions may be appropriate depending on the situation.
Correct Answer is C
Explanation
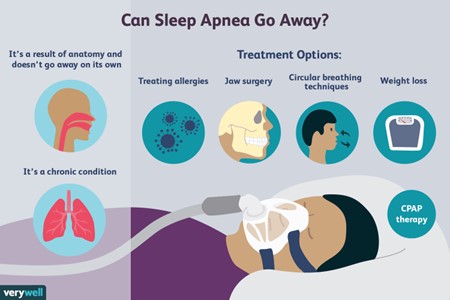
The priority nursing diagnosis for this client should be Risk for injury related to somnambulism. Somnambulism, also known as sleepwalking, can put the client at risk for injury as they may engage in activities while not fully conscious. The client's report of falling asleep while driving and almost being involved in an accident further highlights the potential risk for injury. It is important for the nurse to address this risk and develop a plan to ensure the client's safety.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today