A nurse is teaching a group of newly licensed nurses about the Braden scale. Which of the following responses by a newly licensed nurse indicates an understanding of the teaching?
Each element has a range from one to five points.
The higher the score, the higher the pressure injury risk.
The scale measures six elements.
The client's age is part of the measurement.
The Correct Answer is C
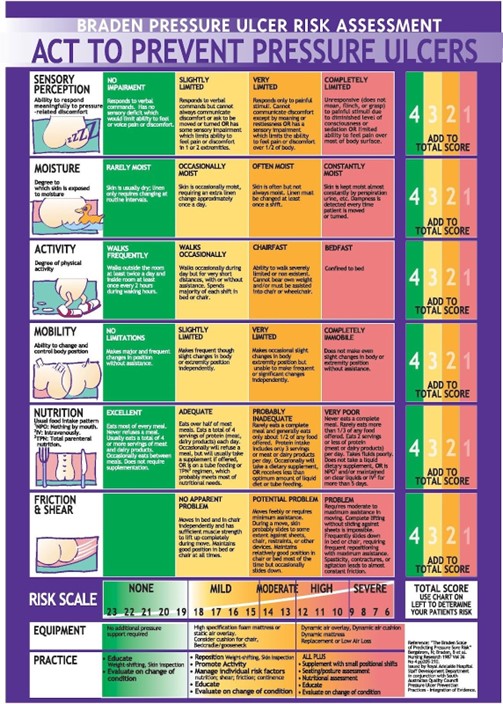
The Braden scale measures six elements: sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each element has a range of one to four points, with a total possible score of 23 points. The lower the score, the higher the risk for pressure injury.
Option a is incorrect because each element has a range from one to four points.
Option b is incorrect because the lower the score, the higher the pressure injury risk.
Option d is incorrect because the client's age is not part of the measurement.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
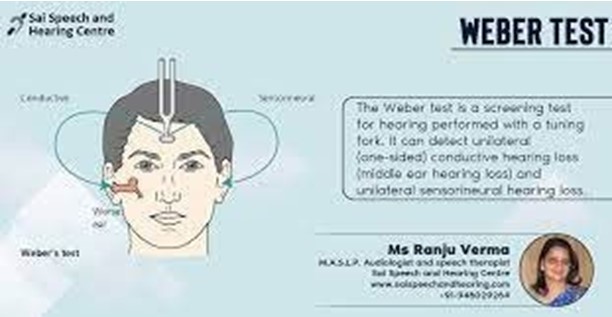
The correct answer is that the nurse should place the base of a vibrating tuning fork on the top of the client's head when performing Weber's test. Weber's test is a screening test for hearing that can detect unilateral (one-sided. conductive hearing loss (middle ear hearing loss) and unilateral sensorineural hearing loss (inner ear hearing loss)².
Options b, c and d are not correct actions for performing Weber's test. Counting how many seconds a client can hear a tuning fork after it has been struck, placing the base of a vibrating tuning fork on the client's mastoid process and moving a vibrating tuning fork in front of the client's ear canals one after the other are not part of Weber's test.
Correct Answer is B
Explanation
The correct answer is that the nurse should expect to find reduced sweat production when performing a skin assessment on an older adult client. As we age, our skin gradually loses its ability to produce sweat and oil, which can result in dry skin¹.
Options a, c and d are not expected findings when performing a skin assessment on an older adult client. Increased skin elasticity, increased production of oils and thickened outer layer of skin are not typical age- related changes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today