A nurse is reinforcing teaching with a parent of an infant who has diaper dermatitis and a new prescription for zinc oxide ointment. Which of the following statements by the parent indicates an understanding of the teaching?
"I will wash off the ointment with each diaper change.”
"I should shake talcum powder onto the reddened areas.”
"I should dry the diaper area with a hair dryer on the lowest setting.”
"I will use moist disposable wipes that are detergent free.”
The Correct Answer is D
Choice A reason:
Washing off the zinc oxide ointment with each diaper change would not be beneficial for the infant's diaper dermatitis. Zinc oxide ointment forms a protective barrier on the skin, and frequent washing could remove this barrier, reducing its effectiveness in promoting healing and protecting the irritated skin.
Choice B reason:
Shaking talcum powder onto the reddened areas is not a suitable approach. Talcum powder can further irritate the skin and worsen the diaper dermatitis. It is best to avoid using talcum powder on an infant's delicate skin.
Choice C reason:
Using a hair dryer, even on the lowest setting, to dry the diaper area is not recommended. The hot air from the hair dryer can be too harsh for the infant's sensitive skin and might exacerbate the irritation. It is safer to let the diaper area air dry naturally or pat it gently with a soft cloth.
Choice D reason:
This is the correct choice. Using moist disposable wipes that are detergent-free is a suitable option for cleaning the infant's diaper area. Detergent-free wipes are gentle on the skin and less likely to cause further irritation. Additionally, keeping the area clean and dry is essential for managing diaper dermatitis, and these wipes can help achieve that without causing harm.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason:
Airborne precautions are implemented for diseases that spread through small airborne particles, such as tuberculosis or measles. These diseases can remain suspended in the air for extended periods and be inhaled by others. Pertussis, also known as whooping cough, is primarily spread through respiratory droplets when an infected person coughs or sneezes, making airborne precautions unnecessary.
Choice B reason:
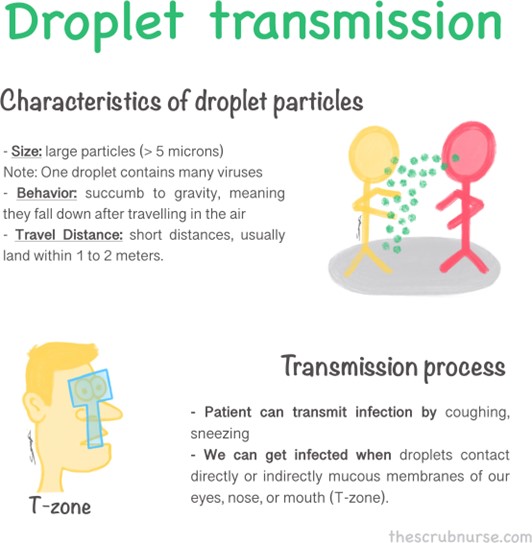
Droplet precautions are appropriate for illnesses that spread through respiratory droplets produced when an infected person talks, coughs, or sneezes. Pertussis falls into this category as it is transmitted mainly through respiratory droplets. By implementing droplet precautions, the nurse will minimize the risk of transmission to others, including healthcare workers and other patients.
Choice C reason:
Standard precautions are the baseline infection prevention practices used for all patients to prevent the spread of infections in healthcare settings. While important, they may not be sufficient to control the transmission of pertussis, as it requires additional measures like droplet precautions due to its specific mode of transmission.
Choice D reason:
Neutropenic precautions are used for patients with compromised immune systems, particularly those with low white blood cell counts (neutropenia). The purpose is to protect these vulnerable individuals from exposure to infectious agents. However, pertussis precautions are different and do not fall under the neutropenic category.
Correct Answer is C
Explanation
"I will reinforce the patch edges with clear tape if they don't lie flat.".
Choice A reason:
Placing a heat pack on the patch to improve adhesion is not recommended. Heat can potentially increase the absorption of the medication and lead to adverse effects. Applying additional heat to the patch can be dangerous and may cause an overdose or other complications.
Choice B reason:
Placing the patch on the back side of the child's arm is not the correct application site for a methylphenidate transdermal patch. The appropriate site for application is typically the hip or the top of the buttocks. The back of the arm may not provide proper absorption and can result in suboptimal medication delivery.
Choice C reason:
This statement indicates an understanding of the teaching. Reinforcing the patch edges with clear tape if they don't lie flat is a recommended step to ensure proper adhesion of the patch. If the edges of the patch lift or don't stick properly, using clear tape can help keep the patch securely in place, ensuring continuous and consistent drug delivery.
Choice D reason:
Leaving the patch in place for no more than 9 hours is incorrect. The duration of wear for a methylphenidate transdermal patch varies depending on the specific brand and formulation. Typically, these patches are designed for 9 to 12 hours of wear, and leaving them on for a shorter duration may result in inadequate symptom control.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today