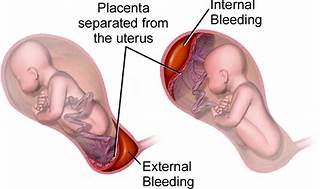
A nurse is reinforcing teaching with a client who is at 34 weeks of gestation and at risk for placental abruption. Does the nurse recognize that which of the following is the most common risk factor for a placental abruption?
Maternal hypertension.
Maternal cocaine use.
Maternal cigarette smoking.
Maternal battering.
The Correct Answer is A
The correct answer is choice A, Maternal hypertension.
Choice A rationale:
Maternal hypertension is widely recognized as the most common risk factor for placental abruption. High blood pressure can cause the placenta to detach from the uterine wall, leading to abruption. In summary, while all the listed factors can contribute to the risk of placental abruption, maternal hypertension stands out as the most common cause, supported by multiple health sources. It’s important for nurses to recognize and manage hypertension in pregnant clients to minimize the risk of this serious complication.
Choice B rationale:
While maternal cocaine use is a significant risk factor for placental abruption due to its vasoconstrictive effects, which can compromise the placental blood flow, it is not as common as maternal hypertension.
Choice C rationale:
Maternal cigarette smoking is also a risk factor for placental abruption. Smoking can lead to a variety of complications in pregnancy, including placental problems, but again, it is less common than hypertension as a cause for abruption.
Choice D rationale:
Maternal battering can lead to trauma which may result in placental abruption. However, it is not considered the most common risk factor when compared to maternal hypertension.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A rationale:
Visual disturbances should be reported to the provider because the client is experiencing headaches, blurred vision, and dizziness, which can be signs of preeclampsia. Preeclampsia is a serious condition that can develop during pregnancy and is characterized by high blood pressure and damage to organs like the liver and kidneys. Visual disturbances may indicate neurological involvement and can pose a risk to both the client and the fetus.
Choice B rationale:
Blood pressure should be reported to the provider due to the client's symptoms and medical history. The client's weight gain, swelling of feet and fingers, and 2+ pitting edema suggest fluid retention, which can be associated with preeclampsia. High blood pressure is a key diagnostic criterion for preeclampsia, and the nurse must monitor it closely to assess the severity of the condition and the potential risk to both the client and the fetus.
Choice C rationale:
Respirations do not appear to be a significant concern based on the information provided. While respiratory status is important to monitor during pregnancy, there are no indications in the scenario to suggest respiratory distress or abnormalities that require immediate reporting to the provider.
Choice D rationale:
Deep tendon reflexes are mentioned in the client's medical history but do not show any immediate signs of concern. Absent clonus and 3+ deep tendon reflexes are within the normal range and not typically alarming during pregnancy. However, the nurse should continue to monitor these reflexes during subsequent visits.
Choice E rationale:
Weight gain is mentioned in the medical history but is not currently a critical finding to report. A 6 lb weight gain over 2 weeks may be considered appropriate for a pregnant client at 32 weeks of gestation, but it should be assessed in conjunction with other symptoms for a comprehensive evaluation.
Correct Answer is ["A","C","D"]
Explanation
Choice A rationale:
The nurse should report the blood pressure findings to the provider because there is a significant increase in both systolic and diastolic blood pressure. At 0900, the blood pressure was 156/90 mm Hg, and at 1000, it increased to 160/96 mm Hg. This significant elevation in blood pressure can be a cause for concern as it may indicate the development of gestational hypertension or preeclampsia, which can be dangerous for both the client and the fetus.
Choice B rationale:
Cerebral manifestations are not mentioned in the nurse's notes or vital signs and are not relevant to the given scenario. Therefore, this choice is not applicable in this case.
Choice C rationale:
The nurse should report the fetal heart rate findings to the provider because it is not included in the vital signs section of the nurse's notes. Monitoring the fetal heart rate is essential to ensure the well-being of the fetus, and any abnormalities or changes in the fetal heart rate should be promptly reported to the healthcare provider for further evaluation.
Choice D rationale:
The nurse should report the respiratory rate findings to the provider. Although the respiratory rate seems to be within the normal range (22/min at 0900 and 21/min at 1000), it is a vital sign that should be closely monitored in pregnant clients. Any sudden changes or abnormalities in the respiratory rate may indicate respiratory distress or other health issues that need medical attention. Choices E and F rationale: Deep tendon reflexes and gastrointestinal assessment findings are not mentioned in the nurse's notes or vital signs. These options are not applicable in this scenario and do not require reporting to the provider.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today