A nurse is reinforcing teaching for a client who has type 1 diabetes mellitus about foot care. Which of the following client statements should indicate to the nurse an understanding of the instructions?
“I put lotion between my toes.”
“I check my feet every day for sores and bruises.”
“I wear sandals in warm weather.”
“I soak my feet in warm, soapy water every night before I go to bed.”
The Correct Answer is B
Choice A: “I put lotion between my toes.” This is incorrect because putting lotion between the toes can create a moist environment that promotes fungal growth and infection. The client should apply lotion to the tops and botoms of the feet, but avoid the areas between the toes.
Choice B: “I check my feet every day for sores and bruises.” This is correct because checking the feet every day for any signs of injury, infection, or ulceration is an important part of foot care for a client who has diabetes mellitus. The client should also report any problems to the provider and seek prompt treatment.
Choice C: “I wear sandals in warm weather.” This is incorrect because wearing sandals can expose the feet to injury, sunburn, or insect bites. The client should wear closed-toe shoes that fit well and protect the feet from trauma and environmental hazards.
Choice D: “I soak my feet in warm, soapy water every night before I go to bed.” This is incorrect because soaking the feet can cause maceration of the skin and increase the risk of infection. The client should wash the feet with mild soap and warm water, but not soak them. The client should also dry the feet thoroughly, especially between the toes.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
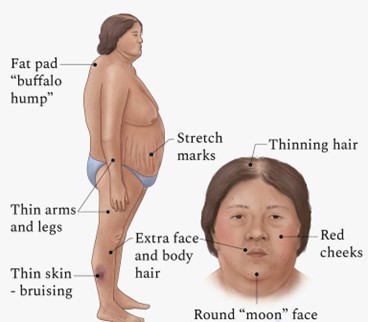
Choice A reason: Weight loss is not a symptom of Cushing’s syndrome. On the contrary, weight gain and obesity are common signs of this condition, especially in the trunk, face and upper back1.
Choice B reason: Diaphoresis, or excessive sweating, is not a symptom of Cushing’s syndrome. It can be caused by other conditions, such as hyperthyroidism, menopause or anxiety.
Choice C reason: Hyperpigmentation, or darkening of the skin, is a symptom of Cushing’s syndrome. It occurs due to increased production of melanin, the pigment that gives color to the skin. Hyperpigmentation can affect any part of the body, but it is more noticeable in areas exposed to friction or pressure, such as the elbows, knees, knuckles and armpits.
Choice D reason: Hypotension, or low blood pressure, is not a symptom of Cushing’s syndrome. In fact, high blood pressure (hypertension) is one of the common symptoms of this condition, due to the effects of cortisol on the cardiovascular system.
Correct Answer is {"A":{"answers":"A,B"},"B":{"answers":"A,B"},"C":{"answers":"B"},"D":{"answers":"B"},"E":{"answers":"A"}}
No explanation
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today