A nurse is reinforcing teaching about self-care with an adolescent client who has infectious mononucleosis with splenomegaly.
Which of the following statements by the client indicates an understanding of the teaching?
“I will take an antibiotic for the next 10 days.”
“I will not play soccer until my doctor tells me I can.”
“I will need to get a varicella booster in 1 month.”
“I will expect the whites of my eyes to turn yellow.”
The Correct Answer is B
“I will not play soccer until my doctor tells me I can.” This statement indicates that the client understands the risk of splenic rupture due to splenomegaly and the need to avoid contact sports until the spleen returns to normal size.
Choice A is wrong because antibiotics are not effective for infectious mononucleosis, which is caused by a virus.
Choice C is wrong because varicella booster is not related to infectious mononucleosis and there is no evidence that the client needs it.
Choice D is wrong because jaundice (yellowing of the eyes and skin) is not a common manifestation of infectious mononucleosis and may indicate another condition such as hepatitis.
Normal ranges for spleen size are 7 to 14 cm in length and 3 to 4 cm in thickness.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Verapamil is a calcium channel blocker that can lower blood pressure and cause dizziness or fainting, especially when standing up from a sitting or lying position. Changing positions slowly can help prevent these symptoms.
Choice A is wrong because palpitations are not an expected side effect of verapamil, but rather a sign of a possible overdose or a serious heart problem that requires medical attention.
Choice C is wrong because verapamil should be taken with food or milk to avoid stomach upset and increase absorption.
Choice D is wrong because verapamil does not cause weight loss, but rather weight gain as a possible side effect.
Increasing calorie intake is not necessary and may worsen other health conditions such as diabetes or high cholesterol.
Correct Answer is B
Explanation
Obturator.
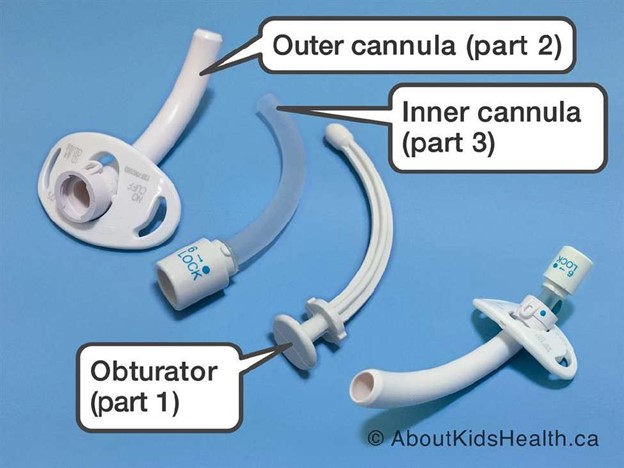
An obturator is a device that is inserted into the tracheostomy tube to guide it through the stoma and prevent tissue damage. It should be removed after the tube is inserted and kept near the bedside in case of accidental decannulation.
Choice A is wrong because povidone-iodine is an antiseptic solution that is not routinely used for tracheostomy care. It can cause skin irritation and damage to the mucous membranes.
Choice C is wrong because an irrigation set is not needed for a tracheostomy tube.
Irrigation can introduce bacteria and increase the risk of infection. It can also cause coughing and bleeding.
Choice D is wrong because hemostats are not used for a tracheostomy tube.
Hemostats are surgical instruments that are used to clamp blood vessels or tissues. They have no role in tracheostomy care.
Some other supplies that the nurse should place in the room are a trach tube the same size as the current tube and one size smaller, a portable suction machine with battery backup, and tubing that connects to the suction machine. Other supplies may include saline solution, syringes, gauze squares, gloves, a trachea tube brush, a waterproof drape, non-woven sponges, pipe cleaners, cotton tipped applicators, a T-drain sponge, twill tape, a trach holder, a speaking valve, a stoma cover, and a nebulizer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today