A nurse is providing teaching to a client who is at 14 weeks of gestation about findings to report to the provider.
Which of the following findings should the nurse include in the teaching
Bleeding gums
Urinary frequency
preeclampsia
faintness upon rising
The Correct Answer is C
This is a sign of preeclampsia, a serious complication of pregnancy that can cause high blood pressure, proteinuria, and seizures.
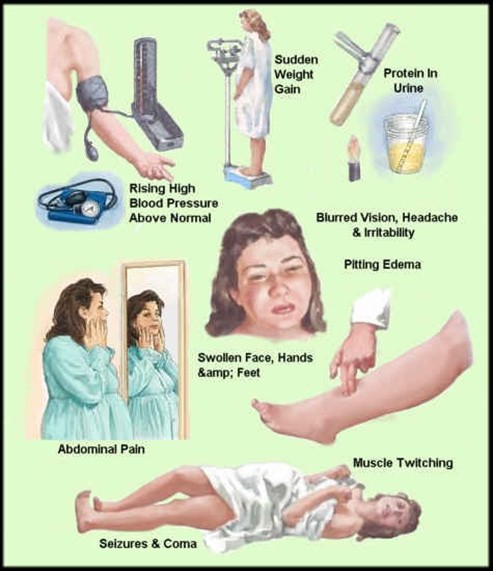
Preeclampsia can affect the placenta, the kidneys, the liver, and the brain of the mother and the fetus. It requires immediate medical attention and may lead to early delivery.
Choice A, bleeding gums, is wrong because it is a common occurrence during pregnancy due to hormonal changes that increase blood flow to the gums. It is not a cause for concern unless it is excessive or accompanied by other symptoms.
Choice B, urinary frequency, is wrong because it is also a normal finding during pregnancy due to the growing uterus putting pressure on the bladder. It is not a sign of infection or kidney problems unless it is associated with pain, burning, or blood in the urine.
Choice D, faintness upon rising, is wrong because it is usually caused by orthostatic hypotension, a drop in blood pressure when changing positions.
This can happen during pregnancy due to the dilation of blood vessels and the increased blood volume. It can be prevented by rising slowly, drinking enough fluids, and avoiding prolonged standing.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The correct answer is B.
Choice A reason: Atrial fibrillation is characterized by a rapid, irregular heartbeat and an absence of distinct P waves on the ECG, which is not indicated by the information provided.
Choice B reason: First-degree AV block is indicated by a prolonged PR interval without affecting the overall heart rate, aligning with the client’s PR interval of 0.24 seconds.
Choice C reason: Premature ventricular contraction would show an abnormal QRS complex on the ECG, which is not mentioned in the scenario.
Choice D reason: Sinus bradycardia is defined by a heart rate less than 60 bpm, which does not apply here as the client’s heart rate is 69/min, within the normal range of 60-100 bpm.
Correct Answer is B
Explanation
Choice A reason
Act as a spokesperson to provide information to the media in inappropriate. During a disaster, the nurse manager or designated hospital spokesperson usually handles communication with the media. The unit nurse's primary focus is on patient care and ensuring the safety and well-being of the clients on their unit.
Choice B reason
Recommending to the provider a list of clients for early discharge is the action that should be taken by the nurse. During a disaster, the responsibility of the unit nurse includes recommending to the healthcare provider a list of clients who may be considered for early discharge. This decision is based on the nurse's assessment of the clients' conditions and the need to create additional capacity for incoming patients who require urgent medical attention.
Choice C reason:
Determining the need for additional providers is inappropriate. The determination of the need for additional providers during a disaster is usually made at a higher level, such as by the nursing supervisor, nurse manager, or hospital administration. The unit nurse may collaborate with the nursing leadership to assess staffing needs and provide input, but the final decision is typically made at a higher level.
Choice D reason
Deciding which clients should be transported for a higher level of care is not the responsibility of the nurse. Decisions about transferring clients for a higher level of care during a disaster are usually made collaboratively among the healthcare team, including the healthcare providers and nursing leadership. The unit nurse may provide valuable input about the clients' conditions, but the decision is not solely the responsibility of the unit nurse.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today