A nurse is planning care for a group of clients. The nurse should expect to witness an informed consent for a client who will undergo which of the following procedures?
Administration of an enema.
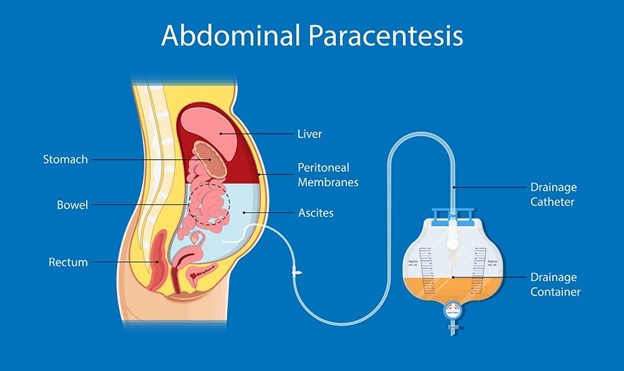
Performance of a paracentesis.
Insertion of an indwelling urinary catheter.
Placement of an NG tube.
The Correct Answer is B
The correct answer is choice B: Performance of a paracentesis.
Choice A rationale:
Administration of an enema does not require informed consent in the same way that invasive procedures do. Enemas are typically considered routine nursing interventions and are not as invasive as the other options.
Choice B rationale:
This is the correct choice. A paracentesis is an invasive procedure that involves puncturing the abdominal cavity to withdraw fluid. Informed consent is required for procedures that carry potential risks, and paracentesis falls into this category due to the risk of complications such as infection, bleeding, or organ injury.
Choice C rationale:
Insertion of an indwelling urinary catheter is a common nursing procedure that, while invasive, does not typically require informed consent. However, the nurse should still explain the procedure to the client and obtain verbal consent, but it's not the same level of formal informed consent required for more invasive procedures.
Choice D rationale:
Placement of an NG tube, although uncomfortable, is not as invasive as a paracentesis. In most cases, NG tube placement is considered a medical or nursing intervention rather than a procedure that necessitates formal informed consent.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The correct answer is choice B: A client who has measles.
Choice A rationale:
Airborne precautions are indicated for diseases that spread via small particles suspended in the air, such as droplets or dust particles that remain in the air for prolonged periods. Pneumonia is primarily spread through larger respiratory droplets and is not considered an airborne disease. Therefore, airborne precautions are not necessary for a client with pneumonia.
Choice B rationale:
Measles is a highly contagious airborne disease caused by the measles virus. It is transmitted through respiratory droplets and can remain in the air for an extended period. Initiating airborne precautions, such as wearing an N95 respirator mask and placing the client in a negative pressure isolation room, is crucial to prevent the spread of measles to healthcare workers and other patients.
Choice C rationale:
Pertussis (whooping cough) is primarily spread through respiratory droplets, similar to pneumonia. While it is a serious bacterial infection, it is not classified as an airborne disease. Thus, airborne precautions are not required for a client with pertussis.
Choice D rationale:
Methicillin-resistant Staphylococcus aureus (MRSA) is mainly spread through direct contact with contaminated surfaces or individuals. Airborne precautions are not necessary for MRSA, as it is not transmitted through the air. Standard precautions, including wearing gloves and gowns, are typically sufficient when caring for a client with MRSA.
Correct Answer is C
Explanation
The correct answer is choicec. Release of personal belongings form.
Choice A rationale:
Completion of an incident report is not typically part of postmortem care documentation unless there was an unusual or unexpected event surrounding the death.
Choice B rationale:
While the name of the nurse certifying the client’s death is important, it is usually documented separately in the death certificate or other official records, not necessarily in the postmortem care documentation.
Choice C rationale:
The release of personal belongings form is crucial as it ensures that the client’s belongings are properly accounted for and handed over to the appropriate person, providing a clear record of what was released and to whom.
Choice D rationale:
Documenting one client identifier at the time of death is important, but it is not specific to postmortem care documentation. Identifiers are generally used throughout the client’s medical record to ensure accuracy and consistency.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today