A nurse is instructing a client’s family members about feeding safety for a client who has dysphagia following a stroke. Which of the following instructions should the nurse include?
Encourage brief exercise before meals to promote appetite.
Encourage the client to take small bites.
Place the client with the head reclined back to facilitate swallowing.
Place food in the affected side of the mouth.
The Correct Answer is B
Choice A reason: Encourage brief exercise before meals to promote appetite. This answer is incorrect because exercise before meals can increase fatigue and decrease appetite in some clients with dysphagia. Exercise can also affect the blood flow to the brain and the muscles involved in swallowing .
Choice B reason: Encourage the client to take small bites. This answer is correct because taking small bites can help the client swallow more easily and reduce the risk of choking or aspiration.
Choice C reason: Place the client with the head reclined back to facilitate swallowing. This answer is incorrect because placing the client with the head reclined back can impair the swallowing mechanism and increase the risk of aspiration. The client should be placed with the head tilted slightly forward to help the food move down the throat.
Choice D reason: Place food in the affected side of the mouth. This answer is incorrect because placing food in the affected side of the mouth can cause the food to remain in the mouth and not be swallowed properly. The client should be encouraged to use both sides of the mouth to chew and swallow food.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Take isoniazid with an antacid. This answer is incorrect because taking isoniazid with an antacid can reduce the absorption and effectiveness of the drug. Isoniazid should be taken on an empty stomach, one hour before or two hours after meals.
Choice B reason: Drink at least 8 ounces of water when you take the pyrazinamide tablet. This answer is incorrect because drinking water with pyrazinamide is not necessary, as this drug does not cause dehydration or kidney problems. However, drinking plenty of fluids is generally recommended for clients with tuberculosis to prevent dehydration and help clear the lungs of secretions.
Choice C reason: Expect your sputum cultures to be negative after 6 months of therapy. This answer is incorrect because expecting sputum cultures to be negative after 6 months of therapy is unrealistic and misleading. The duration of treatment for tuberculosis varies depending on the type and extent of the infection, the drug regimen, and the client's response to the therapy. Some clients may need longer than 6 months to achieve negative sputum cultures.
Choice D reason: Provide a sputum specimen every 2 weeks to the clinic for testing. This answer is correct because providing sputum specimens regularly is important to monitor the effectiveness of the treatment and to determine when the client is no longer infectious.
Correct Answer is C
Explanation
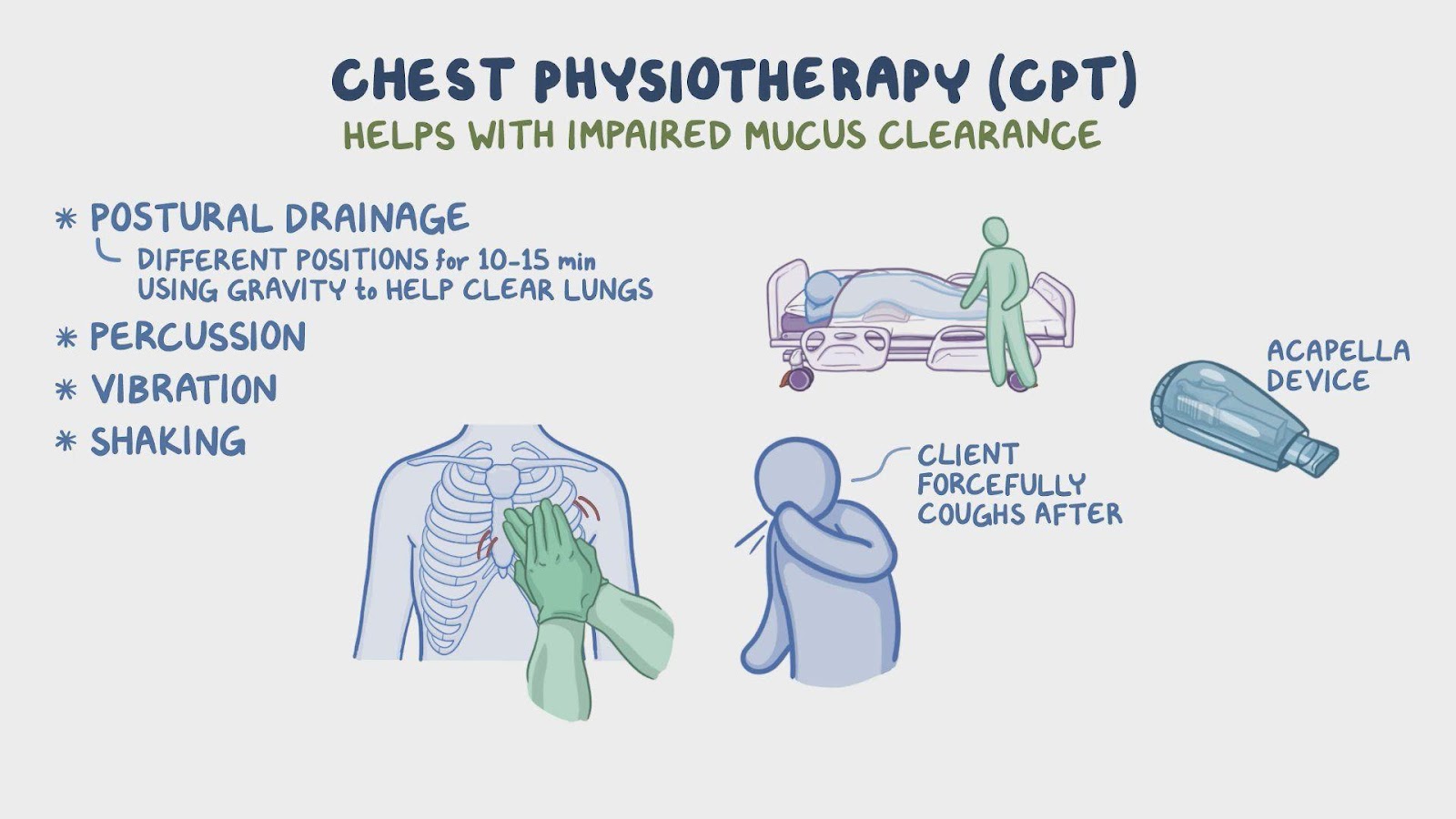
Choice A reason: Performing CPT immediately after the child eats is not a good action for the nurse to plan to take for a child who has cystic fibrosis and a prescription to receive CPT. CPT involves techniques such as percussion, vibration, and postural drainage that help to loosen and remove mucus from the lungs. Performing CPT right after eating can cause nausea, vomiting, or aspiration, especially if the child has gastroesophageal reflux disease (GERD), which is common in cystic fibrosis. The nurse should plan to perform CPT at least 1 hour before or after meals.
Choice B reason: Percussing each lung segment for 15 min is not a necessary action for the nurse to plan to take for a child who has cystic fibrosis and a prescription to receive CPT. Percussion is a technique that involves clapping the chest with a cupped hand to create vibrations that loosen the mucus in the airways. Percussion can be done manually or with a mechanical device. The duration of percussion depends on the amount and location of the mucus, but it is usually done for 3 to 5 min per lung segment. Percussing for 15 min per segment can be excessive and cause bruising, pain, or fatigue.
Choice C reason: Administering albuterol prior to CPT is a beneficial action for the nurse to plan to take for a child who has cystic fibrosis and a prescription to receive CPT. Albuterol is a bronchodilator that helps to relax the smooth muscles of the airways and improve airflow. Administering albuterol before CPT can enhance the effectiveness of the airway clearance techniques by opening up the airways and making it easier to cough up the mucus.
Choice D reason: Performing vibration during the client’s inspirations is not a correct action for the nurse to plan to take for a child who has cystic fibrosis and a prescription to receive CPT. Vibration is a technique that involves applying pressure and shaking the chest wall during exhalation to help move the mucus out of the lungs. Vibration can be done manually or with a mechanical device. Performing vibration during inspiration can interfere with the inhalation of air and oxygen, and reduce the effectiveness of the technique.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today