A nurse is completing a neurovascular check for a client who had an open reduction internal fixation surgery. Which of the following findings should the nurse identify as possible manifestations of compartment syndrome? (Select all that apply)
Absence of pulse
Altered sensation of the toes
Cool skin
Pain relieved by narcotics
Capillary refill 1 second
Correct Answer : A,B,C
The nurse should identify the absence of pulse, altered sensation of the toes, and cool skin as possible manifestations of compartment syndrome. Compartment syndrome is a serious condition that can occur following surgery or injury. It is characterized by increased pressure within a muscle compartment that can lead to decreased blood flow and nerve damage.
Pain relieved by narcotics and capillary refill of 1 second are not manifestations of compartment syndrome. Pain relieved by narcotics is a normal response to pain medication. A capillary refill of 1 second is within the normal range and does not indicate compartment syndrome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
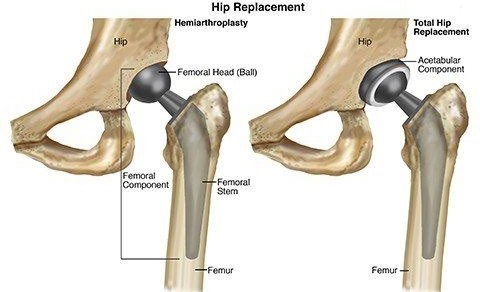
An appropriate action to prevent hip dislocation in a client who is postoperative following a total hip arthroplasty is to place a wedge pillow between the legs. This helps to maintain proper alignment and prevent the legs from crossing or adducting, which can cause hip dislocation.
Placing a trochanter roll against the thigh, placing a sandbag on the lateral calf, and placing a footboard on the bed are not appropriate actions to prevent hip dislocation in this situation. A trochanter roll is used to prevent external rotation of the hip. A sandbag to the lateral calf can help prevent foot drop. A footboard can help prevent plantar flexion contractures.
Correct Answer is A
Explanation
If a nurse is caring for a client who has a spinal cord injury and suspects that the client has autonomic dysreflexia, the first action the nurse should take is to raise the head of the bed. This can help to lower the client's blood pressure and reduce the risk of complications such as stroke.
Checking the client for a fecal impaction is an important step in identifying and treating the underlying cause of autonomic dysreflexia, but it is not the first action the nurse should take.
Checking the client's bladder for distention is an important step in identifying and treating the underlying cause of autonomic dysreflexia, but it is not the first action the nurse should take.
Ensuring that the room temperature is warm is not a priority intervention for a client who has autonomic dysreflexia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today