A nurse is collecting data on the mobility of a client. Which of the following actions should the nurse take first?
Ask the client to stand for 5 seconds.
Ask the client to place their feet on the floor.
Ask the client to sit on the edge of the bed for 2 min.
Ask the client to march in place.
The Correct Answer is C
A) Standing requires more mobility and strength; it's not the first step in assessing mobility.
B) Placing feet on the floor assesses the client's ability to follow instructions and indicates readiness for further mobility assessments but is not the first step compared to sitting on the edge of the bed for 2 minutes.
C) This is the first action that the nurse should take to assess the client's mobility and balance. Sitting on the edge of the bed for 2 min allows the nurse to observe the client's posture, strength, coordination, and ability to maintain equilibrium.
D) This is a more advanced mobility assessment and should come after basic assessments like placing feet on the floor.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
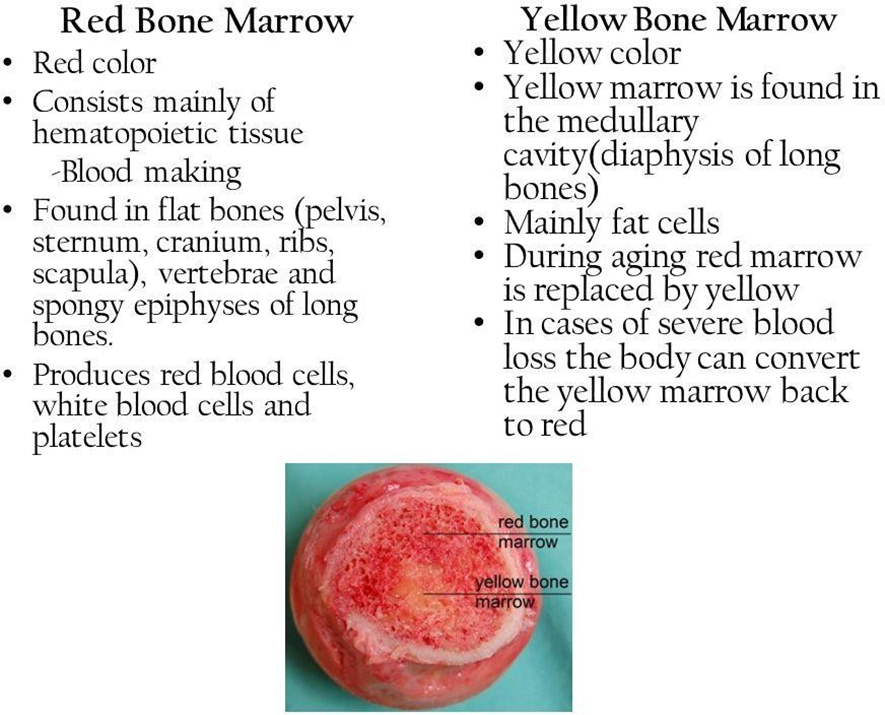
A) While bone marrow does play a role in supporting and protecting bones, its primary function is hematopoiesis.
B) Red bone marrow is responsible for producing various types of blood cells, including white blood cells (leukocytes), red blood cells (erythrocytes), and platelets (thrombocytes).
C) Red bone marrow is primarily involved in hematopoiesis, not calcium storage.
D) This function is more related to the structure and function of joints, ligaments, and muscles, rather than bone marrow.
Correct Answer is D
Explanation
A) This is a medication error, but since it was intercepted before harm occurred, it does not qualify as a sentinel event.
B) While a fall resulting in a fracture is serious, it is not classified as a sentinel event unless the fall results in death, permanent harm, or significant temporary harm.
C) This is a near-miss medication error, which is important to report and investigate but does not meet the criteria for a sentinel event.
D) A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof. Death from sepsis following surgery would qualify as a sentinel event.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today