A nurse is collecting data on a client who has a stage 2 pressure injury. Which of the following findings should the nurse expect?
Intact skin with localized erythema.
Full thickness skin loss with visible bone
Full thickness skin loss with visible adipose tissue.
Partial-thickness skin loss with red tissue in wound bed.
The Correct Answer is D
A. Intact skin with localized erythema:
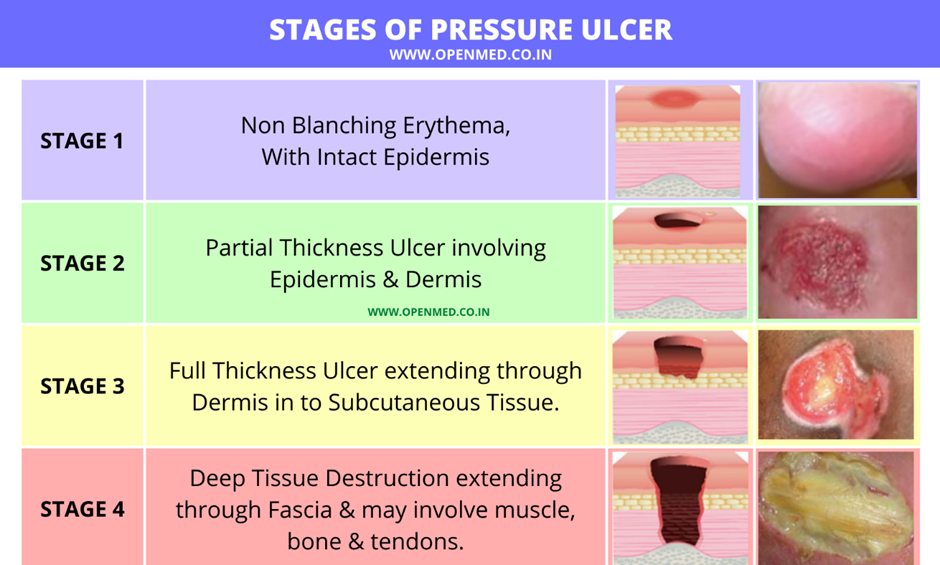
Explanation: This description is more consistent with a stage 1 pressure injury, where there is non-blanchable erythema.
B. Full thickness skin loss with visible bone:
Explanation: This description is more consistent with a stage 4 pressure injury, which involves extensive tissue loss, including exposure of bone.
C. Full thickness skin loss with visible adipose tissue:
Explanation: This finding is characteristic of a stage 3 pressure injury, where the loss of tissue extends down to the subcutaneous layer.
D. Partial-thickness skin loss with red tissue in the wound bed:
Explanation: This description is consistent with a stage 2 pressure injury, where there is partial-thickness skin loss involving the epidermis and possibly the dermis, forming a shallow open ulcer with a red-pink wound bed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. 8.0: An aspirate pH of 8.0 would indicate an alkaline substance. This would not be typical of stomach contents, which are acidic. An alkaline pH might suggest placement in the intestines or respiratory tract.
B. 6.0: While this is less alkaline than 8.0, it is still not within the typical range for stomach contents. Stomach aspirate is generally more acidic.
C. 7.0: A pH of 7.0 is neutral. Stomach contents are typically more acidic, so a neutral pH would not be consistent with correct NG tube placement in the stomach.
D. 4.0: This is within the acidic range and is consistent with the pH of stomach contents. It would be considered an indication of correct NG tube placement in the stomach.
Correct Answer is C
Explanation
A. High-fiber cereals:
High-fiber cereals may not be suitable for a soft diet, as they can be challenging to chew and may not meet the texture requirements of a soft diet.
B. Raw vegetables:
Raw vegetables are generally not recommended for a soft diet, as they can be difficult to chew and digest. Cooking or steaming vegetables can make them softer and more suitable for a soft diet.
C. Ground beef:
This is the correct answer. Ground beef can be included in a soft diet, especially if it is cooked to a tender consistency. It provides a good source of protein while meeting the requirements of a soft-textured diet.
D. Fruit with the skin:
Fruits with skins may pose a challenge for individuals on a soft diet, as the skin can be difficult to chew and swallow. Choosing peeled or canned fruits without skins may be more appropriate.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today