A nurse is collecting data from a client who has increased intracranial pressure and is informed by the charge nurse that the client demonstrates decorticate posturing. Which of the following findings should the nurse expect to observe?
Extension of the extremities
External rotation of the lower extremities
Pronation of the hands
Plantar flexion of the legs
The Correct Answer is D
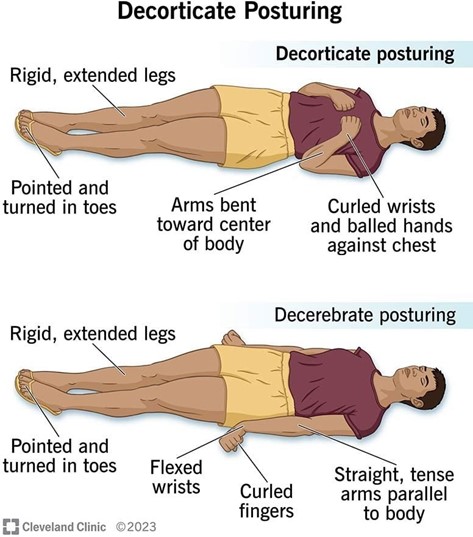
a. Decorticate posturing is marked by the flexion of the arms, with the hands clenched into fists and the legs extended and internally rotated.
b. External rotation of the lower extremities is not a characteristic of decorticate posturing. In decorticate posture, legs are held out straight.
c. Pronation of the hands is characteristic of decerebrate posturing, where the arms are extended and pronated.
d. In decorticate posturing, the lower extremities typically exhibit plantar flexion. Additionally, the upper extremities show flexion of the arms, wrists, and fingers with adduction of the arms.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The knee is a hinge type of joint. When describing range-of-motion exercises, the nurse should explain that the knee is a hinge joint. A hinge joint is a type of synovial joint that mainly allows for flexion and extension (and a small degree of medial and lateral rotation)¹. The knee joint is formed by articulations between the patella, femur, and tibia.
a. The knee is not a pivot joint.
c. The knee is not a ball and socket joint.
d. The knee is not a gliding joint.
Correct Answer is C
Explanation
When contributing to the plan of care for a client to achieve the outcome of functional healing of a fracture, the highest priority nursing intervention to assist in meeting this outcome is to maintain immobilization and alignment for the client. This helps to ensure that the bones are in the correct position to heal properly and can prevent complications such as malunion or nonunion.
a. Promoting independence in activities of daily living for the client is important, but it is not the highest priority intervention for achieving functional healing of a fracture.
b. Providing relief from pain and discomfort for the client is important, but it is not the highest priority intervention for achieving functional healing of a fracture.
d. Providing optimal nutrition and hydration for the client is important, but it is not the highest priority intervention for achieving functional healing of a fracture.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today