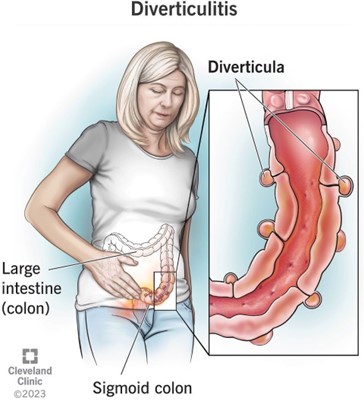
A nurse is collecting data from a client who has diverticular disease. The nurse should expect the client to report abdominal pain in which of the following locations?
Upper left quadrant
Lower left quadrant
Upper right quadrant
Lower right quadrant
The Correct Answer is B
Choice A: Upper left quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper left quadrant of the abdomen contains organs such as the stomach, spleen, pancreas, and part of the colon. Abdominal pain in this area can indicate conditions such as gastritis, peptic ulcer, pancreatitis, splenomegaly, or colon cancer.
Choice B: Lower left quadrant. This is the location where the nurse should expect the client to report abdominal pain who has diverticular disease, which is a condition that involves the formation of pouches or sacs in the wall of the colon. These pouches or sacs are called diverticula, and they can become inflamed or infected, causing diverticulitis. Diverticulitis can cause abdominal pain, fever, nausea, vomiting, and changes in bowel habits. The most common site of diverticula formation and diverticulitis is the sigmoid colon, which is located in the lower left quadrant of the abdomen.
Choice C: Upper right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper right quadrant of the abdomen contains organs such as the liver, gallbladder, duodenum, and part of the colon. Abdominal pain in this area can indicate conditions such as hepatitis, cholecystitis, duodenal ulcer, or colon cancer.
Choice D: Lower right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The lower right quadrant of the abdomen contains organs such as the appendix, cecum, and part of the colon. Abdominal pain in this area can indicate conditions such as appendicitis, Crohn’s disease, or colon cancer.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A: Drinking orange juice regularly. This is a contributing factor to the client’s heartburn because orange juice is acidic and can irritate the esophageal mucosa and lower esophageal sphincter, causing reflux of gastric contents into the esophagus.
Choice B: Eating dinner early in the evening. This is not a contributing factor to the client’s heartburn, but rather a recommended action for the client to prevent heartburn. The client should avoid eating within 3 hours of bedtime to allow for gastric emptying and reduce the risk of reflux.
Choice C: Consuming low-fat meats. This is not a contributing factor to the client’s heartburn, but rather a recommended action for the client to prevent heartburn. The client should avoid high-fat foods, which can delay gastric emptying and increase intra-abdominal pressure, leading to reflux.
Choice D: Sleeping on a large wedge-style pillow. This is not a contributing factor to the client’s heartburn, but rather a recommended action for the client to prevent heartburn. The client should elevate the head of their bed or use a wedge pillow to create an incline that prevents gastric contents from flowing back into the esophagus.
Correct Answer is B
Explanation
Choice A: Increase the client’s sodium intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s sodium intake can worsen fluid retention and exacerbate ascites. The nurse should recommend limiting the client’s sodium intake to less than 2 g per day.
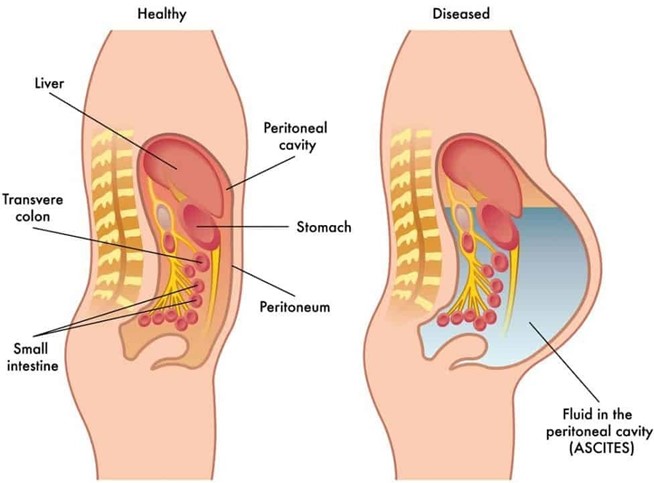
Choice B: Decrease the client’s fluid intake. This is an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Cirrhosis is a chronic liver disease that causes scarring and impaired liver function. Ascites is a complication of cirrhosis that involves the accumulation of fluid in the peritoneal cavity. Decreasing the client’s fluid intake can help reduce fluid retention and prevent further distension of the abdomen and pressure on the diaphragm.
Choice C: Increase the client’s saturated fat intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s saturated fat intake can increase the risk of cardiovascular disease, obesity, and faty liver disease. The nurse should recommend a balanced diet that provides adequate protein, calories, vitamins, and minerals.
Choice D: Decrease the client’s carbohydrate intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Decreasing the client’s carbohydrate intake can cause ketosis, which is a metabolic state that occurs when the body uses fat as a fuel source instead of glucose.
Ketosis can cause nausea, fatigue, headache, and bad breath. The nurse should recommend a moderate carbohydrate intake that provides enough glucose for energy and prevents ketosis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today