A nurse is caring for a toddler who has laryngotracheobronchitis. For which of the following findings should the nurse monitor to detect airway obstruction?
Decreased stridor
Increased restlessness
Decreased heart rate
Decreased temperature
The Correct Answer is B
A. Decreased stridor: Stridor is a high-pitched, noisy breathing sound caused by turbulent airflow through a narrowed or partially obstructed airway. In laryngotracheobronchitis, stridor is often present and may worsen with increasing airway obstruction. Therefore, decreased stridor would not be a typical finding associated with airway obstruction in this condition.
B. Increased restlessness: Increased restlessness can be a sign of worsening respiratory distress and impending airway obstruction. As the child struggles to breathe, they may become increasingly agitated and restless, indicating the need for prompt intervention to ensure adequate oxygenation.
C. Decreased heart rate: Decreased heart rate (bradycardia) is not typically associated with airway obstruction in laryngotracheobronchitis. In fact, the heart rate may increase as a compensatory response to hypoxia and respiratory distress.
D. Decreased temperature: Changes in temperature are not typically associated with airway obstruction in laryngotracheobronchitis. The focus of monitoring in this condition is primarily on respiratory distress and signs of worsening airway obstruction.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
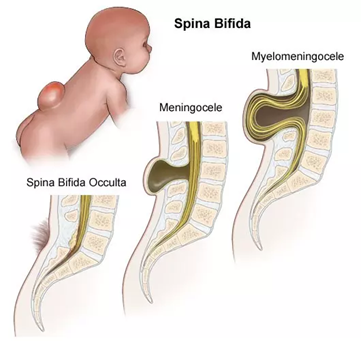
A. Promote maternal-infant bonding: While promoting maternal-infant bonding is essential for the overall well-being of the newborn and family, it may not be the priority in this situation. The immediate focus is on medical management and preventing complications associated with the myelomeningocele.
B. Provide age-appropriate stimulation: Age-appropriate stimulation is important for newborn development, but in the case of a newborn with a myelomeningocele awaiting surgery, the priority is to minimize any potential risk of injury or infection to the exposed neural tissue.
C. Educate the parents about the defect: Education about the myelomeningocele and its long-term implications is crucial for the parents' understanding and ability to care for their child. However, while important, this may not be the priority at the immediate moment.
D. Maintain integrity of the sac: This is the priority nursing goal in caring for a newborn with a myelomeningocele awaiting surgery. The sac covering the exposed neural tissue must be carefully protected to prevent infection and further damage. Measures such as keeping the sac moist with sterile saline dressings and preventing trauma to the area are essential to maintain its integrity.
Correct Answer is A
Explanation
A. Upright: This position allows for better expansion of the lungs and improved ventilation-perfusion matching, as gravity helps the diaphragm move downward and expand the lungs. It is often beneficial for patients with respiratory distress or failure.
B. Supine: While lying flat on the back (supine position) may be comfortable for some patients, it can restrict lung expansion, especially in individuals with compromised respiratory function. This position may not be ideal for maximal lung expansion in this scenario.
C. Prone: The prone position involves lying flat on the abdomen. In some cases, especially in adults with acute respiratory distress syndrome (ARDS), prone positioning has been shown to improve oxygenation by optimizing lung mechanics. However, it may not be practical or comfortable for all patients and is not typically used as a first-line intervention in school-age children with pneumonia.
D. Side-lying: While side-lying positions can sometimes improve lung expansion on the dependent side, it may not be as effective as the upright position in maximizing lung expansion, especially in cases of respiratory failure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today