A nurse is caring for a newly admitted client who has schizophrenia. Which of the following actions is the nurse's priority?
Determine if the client is experiencing command hallucinations.
Arrange for the client to have consistent staff assignments.
Administer lorazepam to the client.
Use the client's name when talking to him.
The Correct Answer is A
Choice A rationale:
Assessing for the presence of command hallucinations is a priority, as they can pose a risk to the client's safety and the safety of others.
Choice B rationale:
Consistent staff assignments can be important for clients with schizophrenia, but immediate safety concerns should take precedence.
Choice C rationale:
Administering medication is not the priority action unless there is a specific reason to do so based on the assessment.
Choice D rationale:
Using the client's name is respectful and helpful, but it is not the priority action in this scenario.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A rationale:
Avoiding temperature extremes can help prevent triggering a sickle cell crisis. Cold temperatures can cause blood vessels to constrict, leading to poor blood flow and increased risk of cell sickling.
Choice B rationale:
Engaging in high-impact exercise might not be recommended, as vigorous exercise can increase the risk of dehydration and oxygen deprivation, potentially triggering a crisis.
Choice C rationale:
Staying well-hydrated by drinking fluids is important, but temperature regulation is a key factor in preventing sickle cell crises.
Choice D rationale:
Receiving the influenza vaccine is recommended for individuals with sickle cell disease to reduce the risk of infections that could trigger a crisis. This statement is incorrect; the client should receive the influenza vaccine unless contraindicated.
Correct Answer is C
Explanation
Choice A rationale:
Ankle swelling can be a common symptom of pregnancy and is not necessarily indicative of a complication.
Choice B rationale:
Gums can become more sensitive during pregnancy, leading to bleeding while brushing teeth. This finding is common and not necessarily indicative of a complication.
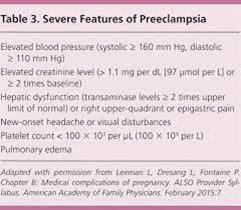
Choice C rationale:
Constant pain in the middle of the upper abdomen can be a sign of preeclampsia, a serious pregnancy complication that requires prompt medical attention.
Choice D rationale:
Feeling dizzy when lying flat on the back (supine hypotension) can be a common discomfort during pregnancy due to pressure on the vena cava. However, it does not necessarily indicate a complication in this context.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today