A nurse is caring for a client with a chest tube. Which action should the nurse take?
Position the collection device below the level of the chest.
Clamp the tube when providing care activities.
Apply an occlusive dressing over the chest tube site.
Empty the chest tube collection chamber every shift.
The Correct Answer is A
Choice A reason: Positioning the collection device below the level of the chest is crucial to ensure proper drainage of air or fluid from the pleural space. This positioning uses gravity to facilitate drainage and prevent backflow into the pleural cavity, which could lead to complications such as pneumothorax or pleural effusion. The collection device should always be kept below the chest level to maintain effective drainage.
Choice B reason: Clamping the chest tube is generally not recommended unless specifically ordered by a physician or during certain procedures. Clamping can lead to a buildup of air or fluid in the pleural space, increasing the risk of tension pneumothorax. It is essential to keep the chest tube unclamped to allow continuous drainage and prevent complications.
Choice C reason: Applying an occlusive dressing over the chest tube site is necessary to prevent air from entering the pleural space and to secure the tube. However, this is not the primary action related to the positioning of the collection device. The occlusive dressing helps maintain the integrity of the chest tube insertion site and prevents infection.
Choice D reason: Emptying the chest tube collection chamber every shift is not a standard practice. The collection chamber should be monitored and emptied as needed based on the volume of drainage and the specific protocols of the healthcare facility. Regular monitoring is essential, but unnecessary emptying can disrupt the closed system and increase the risk of infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Metabolic acidosis is characterized by a decrease in blood pH due to an accumulation of acids or a loss of bicarbonate. It can result from conditions such as diabetic ketoacidosis, renal failure, or severe diarrhea. However, it is not typically associated with opioid overdose. Opioid overdose primarily affects the respiratory system, leading to hypoventilation and respiratory acidosis.
Choice B reason: Respiratory acidosis occurs when there is an accumulation of carbon dioxide (CO2) in the blood due to hypoventilation. Opioid overdose depresses the central nervous system, leading to decreased respiratory rate and depth, which causes CO2 retention. This results in a decrease in blood pH, leading to respiratory acidosis. Symptoms may include confusion, lethargy, and shortness of breath.
Choice C reason: Respiratory alkalosis is characterized by a decrease in blood CO2 levels due to hyperventilation. It can occur in conditions such as anxiety, fever, or high altitude. Opioid overdose, however, causes hypoventilation rather than hyperventilation, making respiratory alkalosis an unlikely outcome.
Choice D reason: Metabolic alkalosis is characterized by an increase in blood pH due to an accumulation of bicarbonate or a loss of acids. It can result from conditions such as prolonged vomiting, diuretic use, or excessive bicarbonate intake. Opioid overdose does not typically lead to metabolic alkalosis. The primary concern with opioid overdose is respiratory depression and the resulting respiratory acidosis.
Correct Answer is C
Explanation
Choice A Reason:
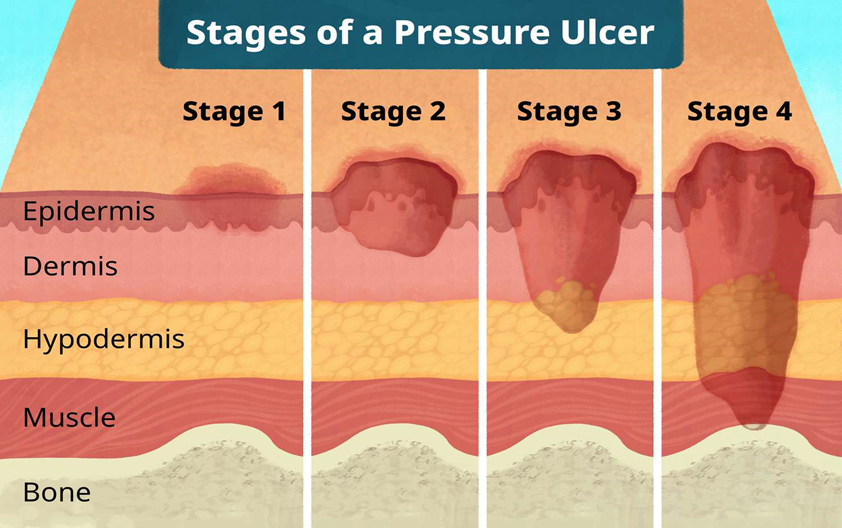
Alginate dressings are typically used for wounds with moderate to heavy exudate because they are highly absorbent. Stage I pressure ulcers do not usually produce exudate, making alginate dressings unnecessary and inappropriate for this type of wound.
Choice B Reason:
Hydrogel dressings are designed to provide moisture to dry wounds and are more suitable for wounds with minimal to no exudate. While they can be used for stage I pressure ulcers, they are not the most common choice as these ulcers do not typically require additional moisture.
Choice C Reason:
Transparent dressings are ideal for stage I pressure ulcers because they protect the skin from friction and shear while allowing for continuous observation of the wound. These dressings maintain a moist environment, which is beneficial for healing, and are easy to apply and remove without causing additional trauma to the skin.
Choice D Reason:
Wet-to-dry gauze dressings are generally used for debridement of necrotic tissue in more advanced wounds. They are not suitable for stage I pressure ulcers, which do not have necrotic tissue and do not require debridement.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today