A nurse is caring for a client who is postoperative following the placement of a colostomy. Which of the following findings indicates that the colostomy is functioning properly?
Passing of flatus
Stoma is pinkish-red
Tolerating a clear liquid diet
Absent bowel sounds
The Correct Answer is B
Choice A reason: Passing of flatus is not a reliable indicator of colostomy function, as it can occur even when there is an obstruction or ischemia in the bowel.
Choice B reason: Stoma is pinkish-red is a sign of a healthy and well-perfused colostomy, as it indicates that the blood supply to the bowel segment is adequate and there is no necrosis or infection.
Choice C reason: Tolerating a clear liquid diet is not a specific indicator of colostomy function, as it does not reflect the amount or consistency of the stool output.
Choice D reason: Absent bowel sounds are not a normal finding for a colostomy, as they can indicate a paralytic ileus or a bowel obstruction, which can cause complications such as distension, pain, or perforation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: This is incorrect. Potassium 4.0 mEq/L is a normal value and does not indicate heart failure.
Choice B: This is correct. Brain natriuretic peptide (BNP) is a hormone that is released by the heart when it is stretched or overloaded. A high level of BNP indicates that the heart is working harder than normal and may have heart failure. A normal BNP level is less than 100 pg/mL, so 275 pg/mL is elevated and suggestive of heart failure.
Choice C: This is incorrect. Sodium 140 mEq/L is a normal value and does not indicate heart failure.
Choice D: This is incorrect. Calcium 9.0 mg/dL is a normal value and does not indicate heart failure.
Correct Answer is A
Explanation
Choice A: This is correct. Phototherapy is a treatment option for psoriasis that involves exposing the skin to ultraviolet light, which can reduce inflammation and slow down the growth of skin cells.
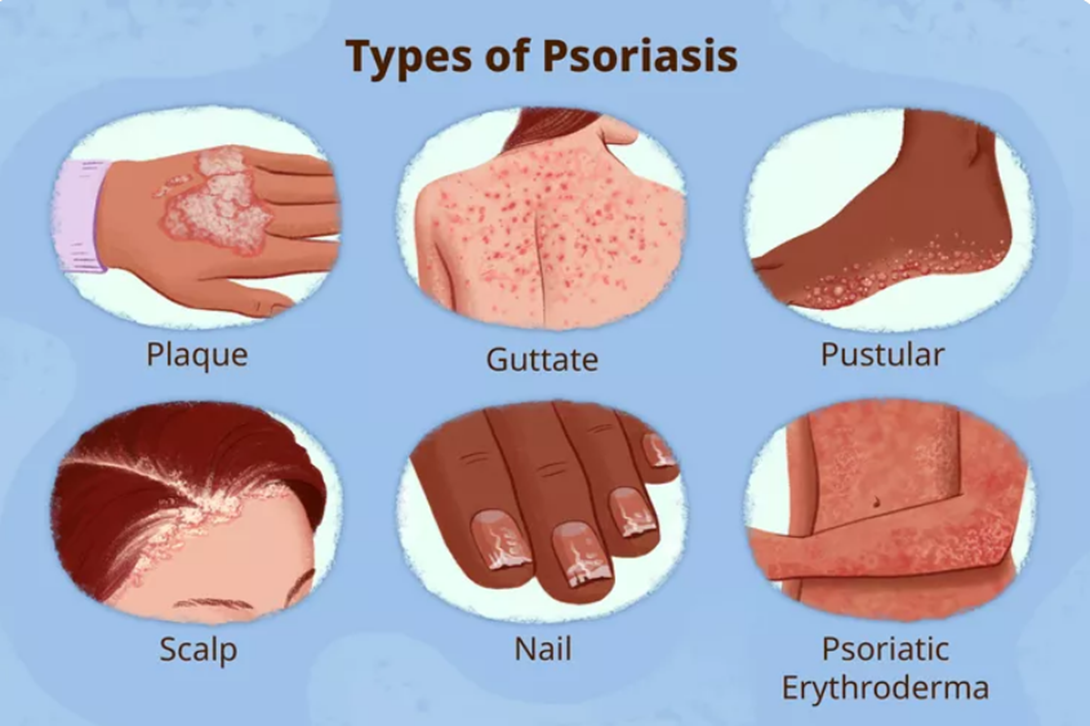
Choice B: This is incorrect. Oil-based ointment is not recommended for psoriasis, as it can clog the pores and worsen the condition.
Choice C: This is incorrect. Dermabrasion is a cosmetic procedure that involves removing the outer layer of skin with a rotating device, which can cause bleeding, infection, and scarring.
Choice D: This is incorrect. Benzoyl peroxide is an acne medication that can dry out and irritate the skin, which can aggravate psoriasis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today