A nurse is caring for a client who is in labor. Which of the following findings should prompt the nurse to reassess the client?
An urge to have a bowel movement during contractions
A sense of excitement and warm, flushed skin
Progressive sacral discomfort during contractions
Intense contractions lasting 45 to 60 seconds
The Correct Answer is A
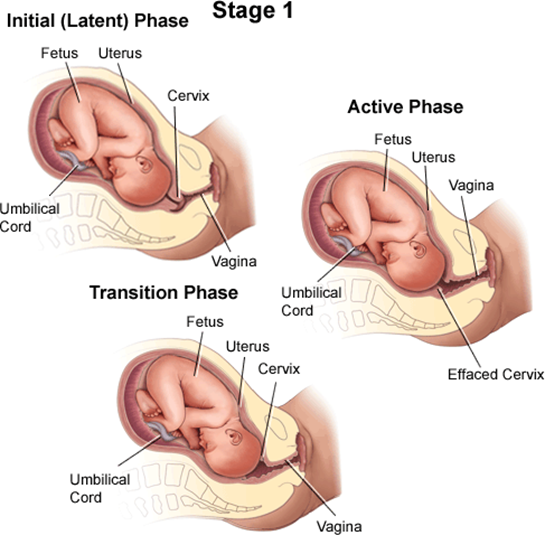
A client who is in labor and reports an urge to have a bowel movement during contractions may be experiencing the transition phase of labor, which is the last and most intense part of the first stage of labor¹². The transition phase occurs when the cervix dilates from 8 to 10 cm and the baby descends into the birth canal¹². The pressure of the baby's head on the rectum can cause a sensation of needing to defecate¹². The transition phase can last from 15 minutes to an hour or more, and it can be accompanied by other signs, such as strong, regular, and painful contractions lasting 60 to 90 seconds; increased bloody show; nausea and vomiting; shaking and shivering; and emotional changes such as irritability, anxiety, or excitement¹²³.
The nurse should reassess the client who reports an urge to have a bowel movement during contractions because this may indicate that the client is close to delivering the baby and needs to be prepared for the second stage of labor, which involves pushing and giving birth¹². The nurse should check the client's cervical dilation, fetal heart rate, and maternal vital signs, and notify the provider if the client is fully dilated or shows signs of fetal or maternal distress¹². The nurse should also support the client's coping strategies, such as breathing techniques, relaxation methods, or pain relief options, and encourage the client not to push until instructed by the provider¹².
b) A sense of excitement and warm, flushed skin are not signs that require reassessment by the nurse. These are normal emotional and physiological responses to labor that reflect increased adrenaline levels and blood flow¹⁴. They do not indicate any complications or imminent delivery.
c) Progressive sacral discomfort during contractions is not a sign that requires reassessment by the nurse. This is a common symptom of labor that results from the pressure of the baby's head on the sacrum and nerves in the lower back¹⁴. It does not indicate any problems or imminent delivery.
d) Intense contractions lasting 45 to 60 seconds are not signs that require reassessment by the nurse. These are typical characteristics of active labor contractions, which occur when the cervix dilates from 4 to 8 cm¹⁴. They do not indicate any complications or imminent delivery.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
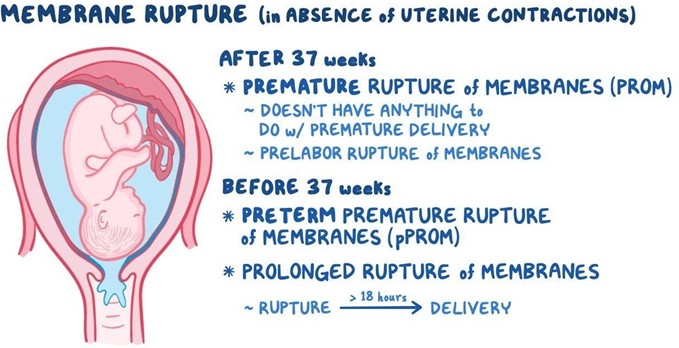
Umbilical cord prolapse is a medical emergency that occurs when the umbilical cord comes out of the uterus with or before the presenting part of the baby. The concern with cord prolapse is that pressure on the cord from the baby will compromise blood flow to the baby. It usually occurs during labor but can occur any time after the rupture of membranes³.
Umbilical cord prolapse can cause fetal hypoxia (lack of oxygen), bradycardia (slow heart rate), acidosis (high acidity in the blood), and death if not treated promptly. The immediate goal of management is to relieve the pressure on the cord and restore blood flow to the baby. The definitive treatment is an emergency cesarean section to deliver the baby as soon as possible¹².
While waiting for the cesarean section, the nurse should take several steps to reduce the risk of fetal
compromise, such as:
- Call for help and notify the provider
- Place the client in a knee-chest, Trendelenburg, or modified Sims position to shift the fetal weight off the
cord
- Exert continuous upward pressure on the presenting part with a sterile gloved hand to lift it away from
the cord
- Administer oxygen to the client at 8 to 10 L/min via a nonrebreather mask
- Administer IV fluids to maintain hydration and blood pressure
- Administer tocolytics (medications that stop uterine contractions) as ordered to reduce cord compression
- Monitor fetal heart rate and uterine activity continuously
- Provide emotional support and reassurance to the client and family
Exerting continuous upward pressure on the presenting part is a critical action that the nurse should take to prevent further cord compression and improve fetal oxygenation. The nurse should insert a sterile gloved hand into the vagina and gently push up on the fetal head or buttocks until delivery. The nurse should not attempt to push the cord back into the uterus or manipulate it in any way, as this could cause more damage or infection¹².
The other options are not actions that the nurse should take:
- a) Place the client in a left-lateral position for 1 hr. after administration. This is not correct because this position does not relieve the pressure on the cord. The client should be placed in a knee-chest, Trendelenburg, or modified Sims position instead.
- b) Initiate oxytocin via continuous IV infusion. This is not correct because oxytocin stimulates uterine contractions, which can worsen cord compression and fetal distress. The nurse should administer tocolytics instead to stop contractions.
- d) Request that the provider insert an intrauterine pressure catheter. This is not correct because an intrauterine pressure catheter is used to measure uterine contractions, not cord prolapse. Inserting a catheter could also increase the risk of infection or injury.
Correct Answer is C
Explanation
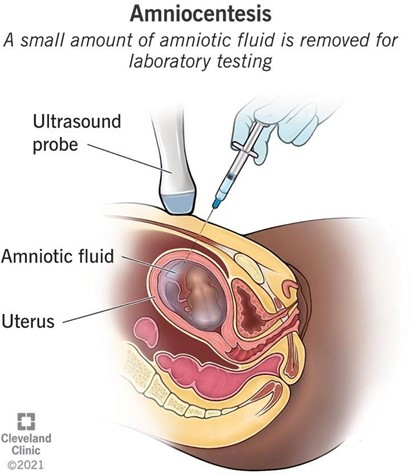
This is because a prescription for an amniocentesis is an indication for the administration of Rho(D) immune globulin (RhIG) to prevent RhD isoimmunization in mothers who are RhD negative¹². RhD isoimmunization is a condition where the mother's immune system produces antibodies against the RhD antigen on the baby's red blood cells, which can cause hemolytic disease of the newborn (HDN)¹². RhIG is a medication that contains antibodies against the RhD antigen, and it works by binding to and destroying any fetal red blood cells that may enter the maternal circulation, preventing the mother from making her own antibodies¹²³. RhIG is usually given to RhD negative mothers during pregnancy and after delivery if the baby is RhD positive¹².
Amniocentesis is a procedure where a needle is inserted into the uterus to obtain a sample of amniotic fluid, which contains fetal cells and other substances⁴. Amniocentesis can be done for various reasons, such as genetic testing, fetal lung maturity assessment, or infection diagnosis⁴. However, amniocentesis also carries a risk of causing bleeding or leakage of amniotic fluid, which can result in fetal-maternal hemorrhage (FMH), where fetal blood cells enter the maternal circulation⁴⁵. FMH can trigger RhD isoimmunization in RhD negative mothers, so they should receive RhIG within 72 hours of the procedure to prevent this complication⁵.
The other options are not correct because:
a) Hyperemesis gravidarum is not an indication for RhIG administration. Hyperemesis gravidarum is a condition where the mother experiences severe nausea and vomiting during pregnancy, which can cause dehydration, electrolyte imbalance, and weight loss. Hyperemesis gravidarum does not affect the blood type or compatibility of the mother and the baby, and does not increase the risk of RhD isoimmunization or HDN.
b) Rh-positive blood test results are not an indication for RhIG administration. Rh-positive blood test results mean that the mother has the RhD antigen on her red blood cells, and therefore she cannot develop antibodies against it¹². Rh-positive mothers do not need RhIG, as they are not at risk of RhD isoimmunization or HDN¹².
d) Anemia is not an indication for RhIG administration. Anemia is a condition where the mother has a low level of hemoglobin or red blood cells, which can cause fatigue, weakness, and shortness of breath. Anemia can have various causes, such as iron deficiency, bleeding, or infection. Anemia does not affect the blood type or compatibility of the mother and the baby, and does not increase the risk of RhD isoimmunization or HDN.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today