A nurse is caring for a client who is immobile. Which prophylactic intervention would be used to prevent complications of immobility?
Applying compression stockings
Raising all side rails
Inserting a urinary catheter
Using friction-reducing devices
The Correct Answer is A
Choice A reason: Applying compression stockings is a key prophylactic intervention to prevent complications of immobility, such as deep vein thrombosis (DVT) and venous thromboembolism (VTE). Compression stockings help improve blood circulation in the legs by applying graduated pressure, which reduces the risk of blood clots forming in the deep veins. This is particularly important for immobile patients who are at higher risk of developing DVT due to prolonged periods of inactivity.
Choice B reason: Raising all side rails is primarily a safety measure to prevent falls and does not directly address the complications of immobility. While it is important for patient safety, it does not have a significant impact on preventing issues like DVT, pressure ulcers, or muscle atrophy. Therefore, it is not considered a prophylactic intervention for immobility-related complications.
Choice C reason: Inserting a urinary catheter is not a prophylactic intervention for preventing complications of immobility. Catheters are used to manage urinary retention or incontinence but can increase the risk of urinary tract infections (UTIs) if not managed properly. They do not address the primary complications associated with immobility, such as DVT or pressure ulcers.
Choice D reason: Using friction-reducing devices is important for preventing pressure ulcers and skin injuries in immobile patients. These devices help minimize friction and shear forces on the skin, which can lead to pressure ulcers. While this is a valuable intervention, it is not as comprehensive as compression stockings in preventing a range of immobility-related complications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Cover
Covering a wound with slough is not an appropriate intervention. Slough is a type of necrotic tissue that can impede the healing process by providing a medium for bacterial growth and preventing the formation of healthy granulation tissue. Simply covering the wound without addressing the slough can lead to infection and delayed healing.
Choice B reason: Clean
Cleaning the wound is a necessary step in wound care, but it is not sufficient on its own to address the presence of slough. While cleaning can help reduce the bacterial load and remove some debris, it does not effectively remove the slough itself. Slough often requires more targeted interventions such as debridement to be effectively managed.
Choice C reason: Debride
Debridement is the most appropriate intervention for a wound with slough. Debridement involves the removal of necrotic tissue, including slough, to promote a clean wound bed and facilitate the healing process. There are several methods of debridement, including autolytic, enzymatic, mechanical, and surgical, each with its own indications and benefits. Removing the slough allows for better assessment of the wound and promotes the formation of healthy granulation tissue.
Choice D reason: Leave Alone
Leaving a wound with slough alone is not advisable. Slough can harbor bacteria and impede the healing process, leading to chronic wounds and potential infection. Without intervention, the wound is unlikely to progress through the normal stages of healing.
Correct Answer is D
Explanation
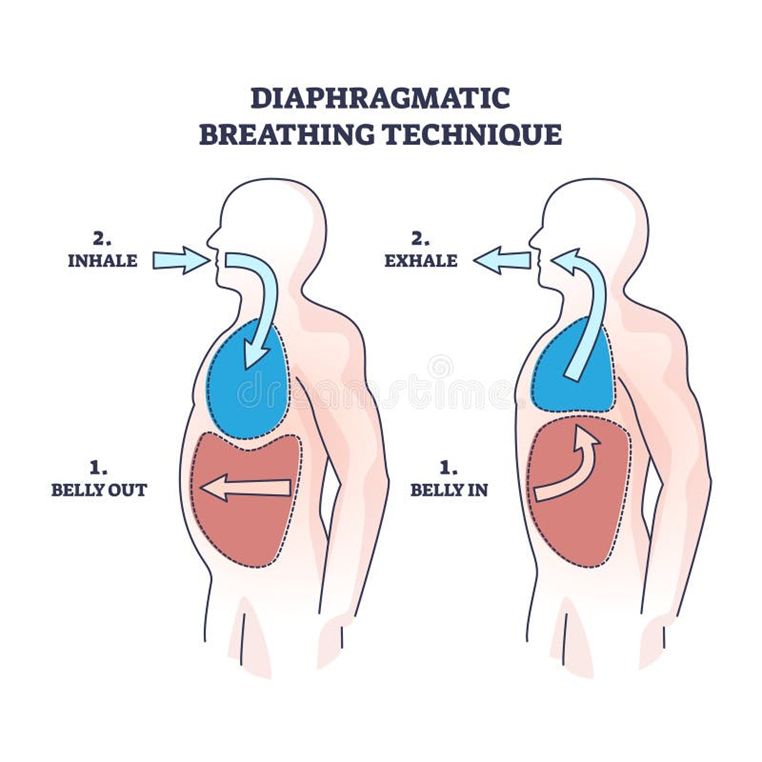
The correct answer is d) Tighten the abdominal muscles while exhaling.
Choice A Reason:
“Raise both shoulders while breathing deeply” is incorrect. Diaphragmatic breathing focuses on using the diaphragm rather than the shoulders. Raising the shoulders can lead to shallow chest breathing, which is less effective for oxygen exchange.
Choice B Reason:
“Inhale through the mouth” is incorrect. For diaphragmatic breathing, it is recommended to inhale through the nose. This helps filter, warm, and humidify the air before it reaches the lungs.
Choice C Reason:
“Exhale through the nose” is incorrect. While exhaling through the nose is beneficial in some breathing exercises, diaphragmatic breathing typically involves exhaling through pursed lips. This technique helps slow down the exhalation and keeps the airways open longer.
Choice D Reason:
“Tighten the abdominal muscles while exhaling” is correct. Tightening the abdominal muscles helps push the diaphragm up, forcing air out of the lungs more efficiently. This action is a key component of effective diaphragmatic breathing.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today