A nurse is caring for a client who has schizophrenia and tells the nurse. "They lie about me all the time and they are trying to poison my food." Which of the following statements should the nurse make?
Why do you think you are being lied about and poisoned?"
You are mistaken. Nobody is lying about you or trying to poison you."
Who is lying about you and trying to poison you?"
You seem to be having very frightening thoughts."
The Correct Answer is D
A. "Why do you think you are being lied about and poisoned?": This question may come across as confrontational or challenging, potentially increasing the client's anxiety or defensiveness. It's important to acknowledge the client's feelings rather than questioning their beliefs directly.
B. "You are mistaken. Nobody is lying about you or trying to poison you.": This statement is dismissive and may cause the client to feel invalidated. It is crucial to acknowledge the client's feelings and experiences, even if they are not based on reality.
C. "Who is lying about you and trying to poison you?": This question may unintentionally reinforce the delusional thinking by suggesting that someone is indeed lying or trying to poison the client. It's essential to avoid validating or encouraging the delusional content.
D. "You seem to be having very frightening thoughts.": This statement acknowledges the client's emotions without directly challenging the delusional content. It shows empathy and creates an open and non-confrontational environment, allowing the client to express their feelings and experiences.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Generalized anxiety disorder and a nursing diagnosis of fear: Generalized anxiety disorder typically involves chronic, excessive worrying and anxiety that is not limited to specific situations or triggers. The sudden and intense symptoms described in the scenario, such as lightheadedness, tremulousness, diaphoresis, tachycardia, and dyspnea, are more indicative of a panic attack rather than generalized anxiety. The nursing diagnosis of fear may not fully capture the acute and intense nature of panic symptoms.
B. Panic disorder and a nursing diagnosis of panic anxiety: This is the correct answer. Panic disorder is characterized by recurrent, unexpected panic attacks, which align with the sudden onset of symptoms described in the scenario. The nursing diagnosis of panic anxiety is appropriate as it addresses the acute distress associated with panic attacks.
C. Pain disorder and a nursing diagnosis of altered role performance: There is no indication of pain being the primary issue in this scenario. The symptoms are more indicative of a panic attack rather than a pain disorder. Additionally, altered role performance is not a priority nursing diagnosis when addressing the acute symptoms of a panic attack.
D. Altered sensory perception and a nursing diagnosis of panic disorder: Altered sensory perception is not the primary issue in this scenario, and it does not specifically address the sudden and intense symptoms described. The focus should be on the panic symptoms and the associated distress, leading to the nursing diagnosis of panic anxiety.
Correct Answer is D
Explanation
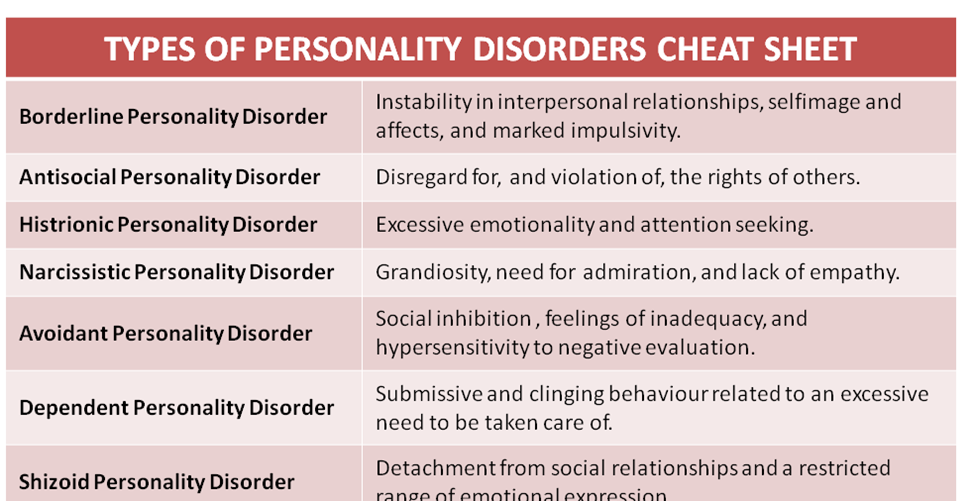
A. Histrionic Personality Disorder:
Individuals with histrionic personality disorder typically seek attention and may be overly dramatic, but self-harm as a response to perceived abandonment is not a characteristic feature.
B. Obsessive-Compulsive Personality Disorder (OCPD):
People with obsessive-compulsive personality disorder are characterized by perfectionism, preoccupation with details, and a desire for control. Michelle's behavior, including self-harm in response to perceived rejection, aligns more closely with borderline personality disorder.
C. Narcissistic Personality Disorder:
While narcissistic individuals may exhibit a sense of superiority and a desire for admiration, self-harm in response to abandonment is not a typical trait of narcissistic personality disorder.
D. Borderline Personality Disorder (BPD):
This personality disorder is characterized by unstable relationships, self-image, and emotions. Individuals with BPD may have intense fears of abandonment and engage in impulsive and self-destructive behaviors. Michelle's perception of being disliked, her claim of superiority, and the self-harming action in response to news of the nurse's vacation are consistent with BPD.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today