A newly admitted client asks. "Why do we need a unit schedule? I'm not going to these groups. I'm here to get some rest." Which is the most appropriate nursing response?
"Group therapy is an economical way of providing therapy to many clients concurrently."
"Group therapy is optional. You can go if you find the topic helpful and interesting."
Group therapy is mandatory. All clients must attend."
"The purpose of group therapy is to learn and practice new coping skills.
The Correct Answer is B
A. "Group therapy is an economical way of providing therapy to many clients concurrently.": While this statement may be true, it does not directly address the client's concerns or provide information about the voluntary nature of group participation.
B. "Group therapy is optional. You can go if you find the topic helpful and interesting.": This is the correct answer. Acknowledging the client's autonomy and providing information about the voluntary aspect of group therapy respects the client's preferences and promotes a collaborative therapeutic relationship.
C. "Group therapy is mandatory. All clients must attend.": This statement is more authoritarian and does not take into account the individual needs and preferences of the client. It is important to involve clients in decisions about their treatment whenever possible.
D. "The purpose of group therapy is to learn and practice new coping skills.": While this statement provides information about the purpose of group therapy, it does not directly address the client's question about the optional nature of attendance.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Maintain consistency of care by open communication to avoid staff manipulation: This is the correct answer. Borderline personality disorder (BPD) clients may engage in splitting behaviors, which involve polarized views of staff as either all good or all bad. Maintaining consistency of care and open communication can help prevent manipulation and ensure fair and transparent interactions.
B. Maintain unit order by the application of autocratic leadership: Autocratic leadership, characterized by a top-down approach with limited input from others, may not be the most effective strategy in this situation. It may lead to resistance from clients and potentially escalate the conflict.
C. Allow the clients to apply the democratic process when developing unit rules: While democratic processes are generally beneficial, allowing clients to unreasonably demand modifications of unit rules without considering the overall impact on the therapeutic environment may not be appropriate. It's important to balance client involvement with maintaining a structured and therapeutic milieu.
D. Allow the client spokesperson to verbalize concerns during a unit staff meeting: While it's important to provide a platform for clients to express concerns, allowing a spokesperson to verbalize concerns during a staff meeting should be done in a manner that maintains order and follows the therapeutic goals of the unit. It should not involve unreasonably demanding modifications without a careful consideration of the impact on the overall treatment milieu.
Correct Answer is A
Explanation
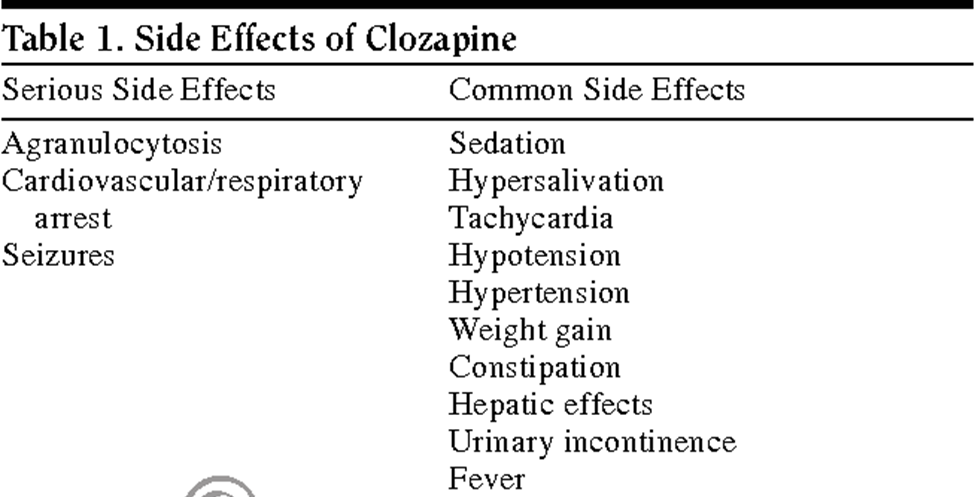
A. WBC count 3,300/mm³.
Clozapine, an atypical antipsychotic medication, is associated with a risk of agranulocytosis, which is a severe reduction in white blood cell (WBC) count. A WBC count of 3,300/mm³ is significantly below the normal range, and it indicates a contraindication to the use of clozapine.
B. Asthma:
Asthma is not a contraindication to clozapine. However, it is important to monitor respiratory function as antipsychotic medications can have side effects related to respiratory function.
C. Hypertension:
Hypertension alone is not a contraindication to clozapine. Clozapine can, however, be associated with some cardiovascular side effects, so blood pressure should be monitored regularly.
D. Fasting blood glucose 120 mg/dL:
An elevated fasting blood glucose level is not a contraindication to clozapine. However, it is important to monitor metabolic parameters as antipsychotic medications, including clozapine, can be associated with metabolic side effects.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today