A nurse is caring for a client who has preeclampsia and is receiving magnesium sulfate. Which of the following clinical findings should the nurse instruct the client to report?
Increased respiratory rate
Increased fetal movement
Increased urinary output
Increased muscle weakness
The Correct Answer is D
When caring for a client with preeclampsia receiving magnesium sulfate, the nurse should instruct the client to report any increased muscle weakness. Magnesium sulfate is a medication commonly used to prevent and treat seizures in clients with preeclampsia. However, one of the side effects of magnesium sulfate is muscle weakness. If the client experiences an increase in muscle weakness, it could indicate magnesium toxicity, which requires immediate medical attention.
Option a) Increased respiratory rate is not typically associated with magnesium sulfate administration. However, respiratory depression is a potential side effect, so a decreased respiratory rate should be reported.
Option b) Increased fetal movement is generally considered a positive sign of fetal well-being and is not a concern that needs to be reported.
Option c) Increased urinary output is not typically a concerning finding. In fact, maintaining adequate urine output is desired in clients with preeclampsia to ensure proper kidney function. However, a sudden decrease in urinary output or signs of dehydration should be reported.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A nonstress test (NST) is a test in pregnancy that measures fetal heart rate in response to movement and contractions²³. A normal nonstress test will show a baseline fetal heart rate between 110 and 160 beats per minute with moderate variability (5- to 25-interbeat variability) and 2 qualifying accelerations in 20 minutes with no decelerations³⁴. An acceleration is defined as an increase in the fetal heart rate of at least 15 beats per minute above the baseline for at least 15 seconds²³⁴.
A nonstress test can be affected by uterine contractions, which can cause fetal heart rate decelerations or reduced variability²³. Uterine contractions can also indicate preterm labor or placental abruption, which are serious complications that require intervention². Therefore, if the nurse observes three or more uterine contractions within a 20-minute period during a nonstress test, they should intervene by notifying the provider, assessing the patient for signs of labor or bleeding, and preparing for further evaluation or treatment²⁵.
The other options are not correct because they do not require intervention by the nurse:
a) One acceleration of the FHR within a 20-min period is not enough to meet the criteria for a reactive nonstress test, but it does not indicate fetal distress or compromise. The nurse should continue monitoring the fetal heart rate for another 20 minutes or until two accelerations are observed²³⁴.
b) Uterine contractions lasting 20 to 30 seconds each are normal and expected during pregnancy, especially in the third trimester. They are called Braxton Hicks contractions and they help prepare the uterus for labor. They are usually painless and irregular, and do not cause cervical changes. They do not require intervention by the nurse unless they become frequent, intense, or painful².
d) An FHR that peaks 20 beats above the baseline is considered an acceleration and is a sign of fetal well- being. It does not require intervention by the nurse unless it is associated with decelerations or reduced variability²³⁴.
Correct Answer is D
Explanation
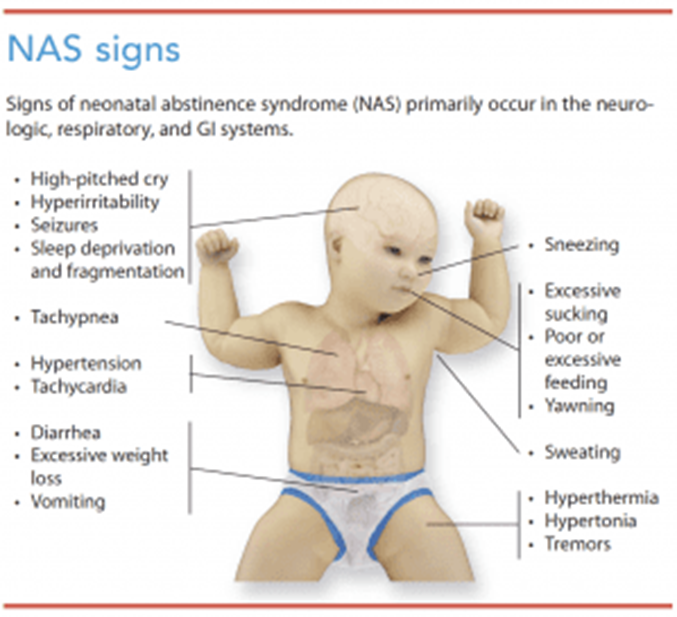
Neonatal abstinence syndrome (NAS) occurs in newborns who were exposed to addictive substances, such as opioids, during pregnancy. Infants with NAS may experience withdrawal symptoms and can be hypersensitive to stimuli. Therefore, it is important to minimize unnecessary handling to help reduce stimulation and discomfort for the newborn.
Option a) Swaddling the newborn with his legs extended may increase discomfort for a newborn with NAS. It is often recommended to swaddle newborns with NAS in a flexed position to provide a sense of security and comfort.
Option b) Maintaining eye contact during feedings may be overwhelming for a newborn with NAS. Maintaining a calm, quiet environment during feedings can help reduce overstimulation and improve feeding success.
Option c) Scheduling larger volume feedings at less frequent intervals may not be appropriate for a newborn with NAS. These infants may have poor feeding tolerance and may benefit from smaller, more frequent feedings to avoid overwhelming their gastrointestinal system.
Therefore, option d) Plan care to minimize handling of the newborn is the correct action to take when caring for a newborn with neonatal abstinence syndrome. It helps reduce stimulation and discomfort for the newborn.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today