A nurse is caring for a client who has major depressive disorder and is refusing their medication. The client's family suggests placing the client's medication in their food. Which of the following actions should the nurse take?
Schedule the medication at meal times.
Request the family talk to the provider about administering the medication by injection.
Inform the family that the client has the right not to take the medication.
Ask the family what foods the client likes.
The Correct Answer is C
The nurse should inform the family that the client has the right to refuse medication. It is important to
respect the client's autonomy and right to make decisions about their own care.
a) Scheduling the medication at meal times does not address the issue of the client refusing their medication.
b) Requesting that the family talk to the provider about administering the medication by injection may be an option, but it does not address the issue of informed consent.
d) Asking the family what foods the client likes does not address the issue of informed consent and could be seen as a way to deceive the client into taking their medication.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
d. Remove the IV catheter.
Explanation:
The correct answer is d. Remove the IV catheter.
If the nurse realizes that the incorrect IV solution is infusing, it is essential to take prompt action to prevent harm to the client. Removing the IV catheter is the appropriate course of action to stop the infusion of the incorrect solution.
Option a, completing an incident report, may be necessary after the immediate situation has been addressed, but it should not be the nurse's first action. The priority is to stop the incorrect solution from infusing.
Option b, allowing the current solution to finish infusing and then changing the bag, is not the correct action. Continuing the infusion of the incorrect solution can potentially harm the client and must be stopped immediately.
Option c, documenting that an error occurred in the client's medical record, is important, but it should be done after taking immediate action to stop the incorrect solution from infusing. Documentation should include the details of the incident, any actions taken, and the client's response.
By promptly removing the IV catheter, the nurse stops the infusion of the incorrect solution and prevents further harm to the client. Afterward, the nurse should assess the client for any adverse effects, inform the appropriate healthcare providers, and follow the facility's policies and procedures for reporting incidents and documenting the error.
Correct Answer is C
Explanation
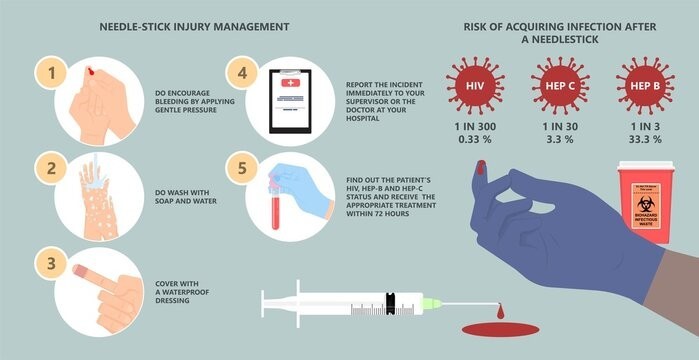
c. Dispose of the used needle immediately in a sharps container.
The nurse should dispose of the used needle immediately in a sharps container to reduce the risk of a needlestick injury. Sharps containers are specifically designed for the safe disposal of needles and other sharp objects. By placing the used needle directly into a sharps container, the nurse eliminates the need for handling or manipulating the needle further, reducing the risk of accidental needlestick injuries.
Explanation for the other options:
a. Place a cap holder securely on the used needle before disposal: Cap holders are not recommended for securing used needles before disposal. They may not provide adequate protection against needlestick injuries and can potentially increase the risk of accidental needlesticks when atempting to secure the cap holder.
b. Recap the needle for disposal later: Recapping the needle increases the risk of a needlestick injury. It is generally not recommended to recap needles after use, as it poses a greater risk of accidental puncture.
d. Detach the used needle and dispose of it promptly: Detaching the needle from the syringe before disposal is not recommended, as it increases the risk of a needlestick injury. It is safer to dispose of the needle and syringe as a unit in a sharps container to minimize the risk of accidental puncture.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today