A nurse is caring for a client who has leukemia. Which of the following findings is the highest priority for the nurse to report to the provider?
Weight loss
Fatigue
Dysuria
Elevated temperature
The Correct Answer is D
Choice A: This is incorrect because weight loss is not the highest priority finding for the nurse to report to the provider. Weight loss can be a common symptom of leukemia due to decreased appetite, increased metabolism, or malabsorption.
Choice B: This is incorrect because fatigue is not the highest priority finding for the nurse to report to the provider. Fatigue can be a common symptom of leukemia due to anemia, infection, or poor nutrition.
Choice C: This is incorrect because dysuria is not the highest priority finding for the nurse to report to the provider. Dysuria can indicate a urinary tract infection, which can be treated with antibiotics and fluids.
Choice D: This is correct because elevated temperature is the highest priority finding for the nurse to report to the provider. Elevated temperature can indicate a serious infection, which can be life-threatening for a client who has leukemia and a compromised immune system.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: This is incorrect because placing the client in the Sims' position is not necessary for a colposcopy. The nurse should place the client in the lithotomy position, which allows better visualization of the cervix and vagina.
Choice B: This is incorrect because inserting a tampon following the procedure can interfere with healing and increase the risk of infection. The nurse should instruct the client to avoid using tampons, douches, or vaginal creams for at least a week after the procedure.
Choice C: This is correct because instructing the client to avoid sexual intercourse until the cervix is healed can prevent bleeding, infection, and trauma to the cervix. The nurse should advise the client to abstain from sexual activity for at least a week or until advised by the provider.
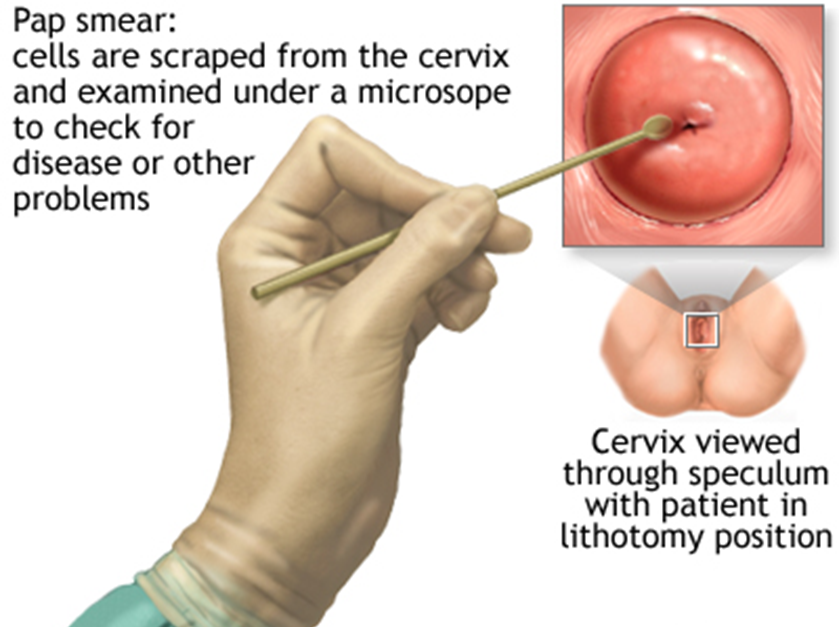
Choice D: This is incorrect because reinforcing teaching that the procedure involves dilation of the cervix can cause anxiety and discomfort for the client. The nurse should explain that the procedure does not require dilation of the cervix, but rather involves applying a speculum and using a microscope to examine the cervix and take tissue samples if needed.
Correct Answer is D
Explanation
Choice A reason: Filling the pad with sterile water is not necessary, as tap water can be used for an aquathermia pad without increasing the risk of infection or contamination.
Choice B reason: Using safety pins to secure the pad in place is not appropriate, as they can puncture or damage the pad and cause leakage or electric shock.
Choice C reason: Applying the pad for 45 min at a time is not recommended, as it can cause skin burns or tissue damage due to prolonged exposure to heat. The nurse should apply the pad for no more than 20 min at a time and check the skin frequently for signs of redness or blistering.
Choice D reason: Covering the pad prior to use is an important action, as it can prevent direct contact between the pad and the skin and reduce the risk of burns or irritation. The nurse should use a towel or a cloth to cover the pad before applying it to the affected area.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today