A nurse is caring for a client who has hyperparathyroidism. Based on this diagnosis, the nurse should monitor the client for which of the following complications?
Dysphagia
Pathologic fractures
Fluid retention
Impaired skin integrity
The Correct Answer is B
Choice A: Dysphagia. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Dysphagia is difficulty swallowing, which can be caused by disorders of the esophagus, throat, or nervous system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
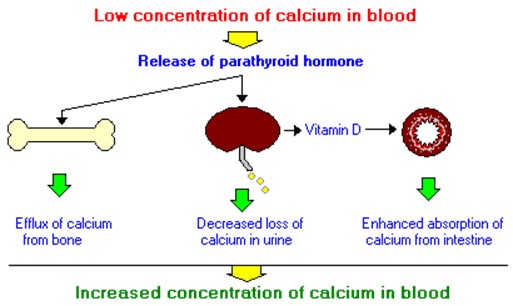
Choice B: Pathologic fractures. This is a complication that the nurse should monitor the client for who has hyperparathyroidism, which is a condition that occurs when the parathyroid glands produce too much parathyroid hormone (PTH). PTH regulates calcium and phosphorus levels in the blood and bones. Hyperparathyroidism can cause hypercalcemia, which is a high level of calcium in the blood, and hypophosphatemia, which is a low level of phosphorus in the blood. These imbalances can lead to bone resorption, which is the breakdown of bone tissue and release of calcium into the blood. Bone resorption can weaken the bones and increase the risk of pathologic fractures, which are fractures that occur due to disease or injury to the bone.
Choice C: Fluid retention. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Fluid retention is excess fluid accumulation in the body, which can be caused by disorders of the heart, kidney, liver, or lymphatic system. It is not related to hyperparathyroidism or calcium and phosphorus levels.
Choice D: Impaired skin integrity. This is not a complication that the nurse should monitor the client for who has hyperparathyroidism. Impaired skin integrity is damage or loss of skin tissue, which can be caused by trauma, infection, inflammation, or pressure. It is not related to hyperparathyroidism or calcium and phosphorus levels.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: Place the client on bedrest. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Placing the client on bedrest can increase the risk of complications such as thromboembolism, pressure ulcers, and muscle atrophy. The nurse should encourage the client to perform gentle exercises and change positions frequently.
Choice B: Apply warm blankets. This is an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Hypothyroidism is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. Thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects the energy expenditure and body temperature. Myxedema is a severe form of hypothyroidism that causes swelling of the skin and tissues due to accumulation of mucopolysaccharides. Applying warm blankets can help maintain the client’s body temperature and prevent hypothermia, which is a low body temperature.
Choice C: Check the client for weight loss. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Checking the client for weight loss can indicate hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone.
Hyperthyroidism can cause weight loss due to increased metabolic rate and appetite. The nurse should check the client for weight gain, which can indicate hypothyroidism due to decreased metabolic rate and fluid retention.
Choice D: Limit high-fiber foods. This is not an intervention that the nurse should include in the plan of care for a client who has hypothyroidism with myxedema. Limiting high-fiber foods can cause constipation, which can worsen hypothyroidism symptoms such as bloating, abdominal pain, and fatigue. The nurse should encourage the client to eat high-fiber foods, such as fruits, vegetables, and whole grains, to promote bowel regularity and prevent constipation.
Correct Answer is D
Explanation
Choice A: Bradycardia. This is not a manifestation of gastrointestinal perforation, but rather a sign of vagal stimulation, which can occur in response to gastric distension, vomiting, or suctioning. Vagal stimulation can slow down the heart rate and lower the blood pressure.
Choice B: Hyperactive bowel sounds. This is not a manifestation of gastrointestinal perforation, but rather a sign of increased intestinal motility, which can occur in response to inflammation, infection, or irritation of the gastrointestinal tract. Hyperactive bowel sounds are loud, high-pitched, and frequent.
Choice C: Report of epigastric fullness. This is not a manifestation of gastrointestinal perforation, but rather a sign of delayed gastric emptying, which can occur in response to gastric outlet obstruction, gastroparesis, or pyloric stenosis. Epigastric fullness is a feeling of pressure or discomfort in the upper abdomen after eating.
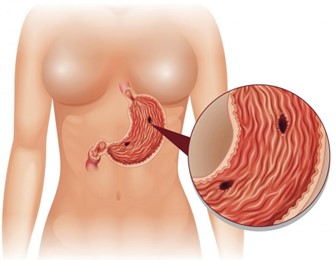
Choice D: Severe upper abdominal pain. This is a manifestation of gastrointestinal perforation, which is a life-threatening complication of peptic ulcer disease. Peptic ulcer disease is a condition that causes erosion and ulceration of the mucosal lining of the stomach or duodenum. If the ulcer penetrates through the wall of the gastrointestinal tract, it can cause perforation, which is a hole that allows gastric contents to leak into the peritoneal cavity. This can cause peritonitis, which is an inflammation and infection of the peritoneum. Peritonitis can cause severe upper abdominal pain, which may radiate to the shoulder or back. The pain may be sudden, sharp, and constant.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today