A nurse is caring for a 4-year-old child who had an incident of bedwetting during hospitalization. The child's parents expresses concern about the incident. Which of the following responses should the nurse make?
"I know this can be embarrassing. I have kids myself so I understand, and it doesn't bother me."
"Children who are hospitalized often regress. The toileting skills will return when your child is feeling better."
"I will discuss your child's loss of bladder control with the provider."
"Why is she wetting the bed in the hospital? She must wet the bed at home."
The Correct Answer is B
A. "I know this can be embarrassing. I have kids myself so I understand, and it doesn't bother me."
This response acknowledges the child's feelings and reassures the parents that bedwetting is a common occurrence, especially during hospitalization. It also demonstrates empathy by sharing a personal experience. However, it may not address the parents' concerns about their child's bedwetting or provide information on how to manage it.
B. "Children who are hospitalized often regress. The toileting skills will return when your child is feeling better."
This response provides an explanation for the bedwetting incident, reassuring the parents that it is a common response to hospitalization and will likely resolve once the child feels better. It offers support and normalization of the behavior, which can help alleviate the parents' concerns.
C. "I will discuss your child's loss of bladder control with the provider."
This response indicates that the nurse will address the issue with the healthcare provider, which is appropriate if further evaluation or intervention is needed. However, it may not directly address the parents' concerns or provide immediate reassurance.
D. "Why is she wetting the bed in the hospital? She must wet the bed at home."
This response may come across as accusatory or judgmental, which can increase parental anxiety or guilt. It does not provide reassurance or support to the parents and does not address the child's immediate needs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
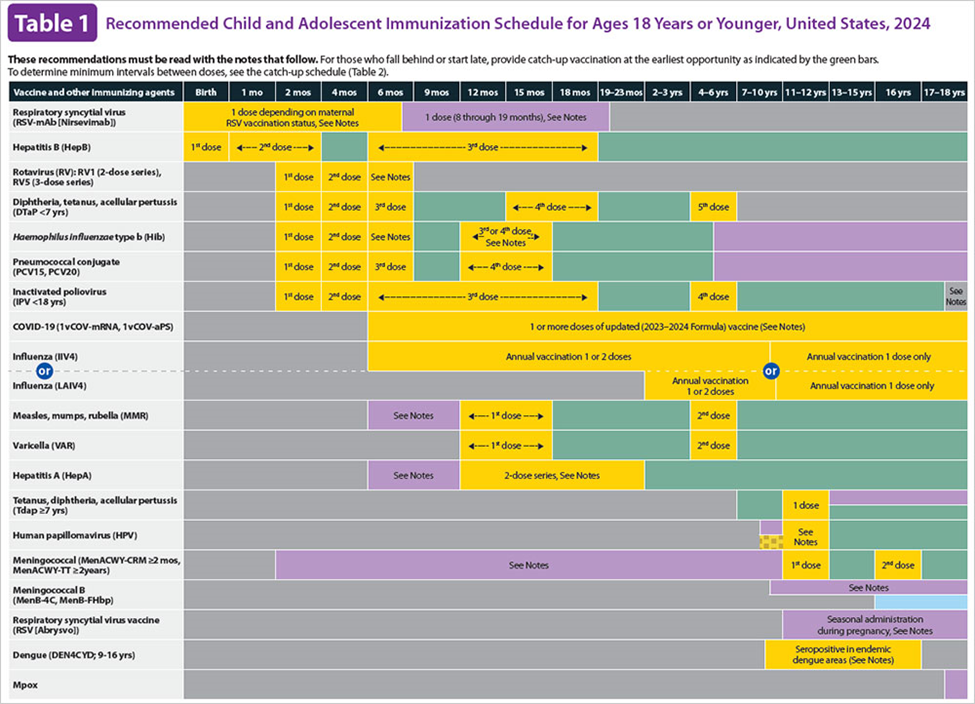
A. Influenza:
The influenza vaccine is typically administered annually starting at 6 months of age. It helps protect against seasonal influenza viruses and is usually recommended during the fall or winter months.
B. Rotavirus:
The rotavirus vaccine is routinely administered to infants starting at 2 months of age, with additional doses given at 4 and 6 months of age. It helps prevent rotavirus infection, which can cause severe diarrhea and vomiting in infants and young children.
C. Measles, mumps, rubella (MMR):
The MMR vaccine is typically administered around 12-15 months of age, with a second dose given at 4-6 years of age. It helps protect against measles, mumps, and rubella, which are contagious viral infections that can cause serious complications.
D. Varicella (VAR):
The varicella vaccine, also known as the chickenpox vaccine, is usually administered around 12-15 months of age, with a second dose given at 4-6 years of age. It helps prevent chickenpox, a highly contagious viral infection characterized by a rash and fever.
Correct Answer is D
Explanation
A. Monitor the client's hemoglobin level: Monitoring the client's hemoglobin level is not relevant during a seizure. Seizures typically do not directly affect hemoglobin levels, so this action is not appropriate.
B. Restrain the client's extremities: Restraint is generally not recommended during a seizure unless absolutely necessary for the safety of the client or others. Restraint can potentially cause injury to the client and increase agitation during the seizure.
C. Place the client in a prone position: Placing the client in a prone (face-down) position during a seizure is not recommended. This position may increase the risk of airway obstruction and compromise the client's ability to breathe effectively.
D. Record the time and length of the seizure: This is the correct answer. During a seizure, the nurse should prioritize ensuring the safety of the client and others. After ensuring safety, the nurse should document important details about the seizure, including the time it began and ended, as well as any observed symptoms or behaviors. This documentation can provide valuable information for the client's healthcare team and help guide future treatment decisions.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today