A nurse is assisting with the care of a client.
Nurses' Notes
1000
Client states, "I am tired of undergoing treatment because it doesn't seem to be working." Client states, "I hope I am just constipated." Appendectomy scar on right lower quadrant. Abdomen is soft, tender in right lower quadrant, bowel sounds present in all four quadrants.
1200
Surgeon has notified the client that surgical removal of the mass is advisable due to the client's history of metastasis and ongoing treatment failure. The client and their partner want to discuss end-of-life care. Client states, "I am unsure what it means to have a living will or a do-notresuscitate order." The client's partner states, " don't understand what power of attorney means. Both client and partner indicate that they might wish to decline further treatment as well as further fesaving measures should they become necessary. The partner states "How can we be sure that our decision about care will be honored?"
Select the 4 responsibilities the nurse has in relation to the client's advance directives.
Communicate advance directives status via the medical record and shift report.
Document that the provider discussed do-not-resuscitate status with the client
Provide the client with written information about advance directives
Instruct the client that an advance directive is a legal document and must be honored by care providers
Inform the client that an advance directive discontinues further care.
Facilitate a power of attorney for health care document.
Correct Answer : A,B,C,F
The nurse is responsible for educating the client and their partner about advance directives and facilitating their decision-making process. Advance directives are legal documents that allow the client to express their preferences for medical care and treatments at the end of life.
They also enable the client to appoint a health care proxy, who is a person who can make health care decisions for the client if they are unable to do so themselves.
The nurse should provide the client with written information about advance directives, document that the provider discussed do-notresuscitate status with the client, and communicate advance directives status via the medical record and shift report.
The nurse should not instruct the client that an advance directive is a legal document and must be honored by care providers, as this may imply coercion or limit the client's right to change their mind.
The nurse should also not inform the client that an advance directive discontinues further care, as this is inaccurate and may discourage the client from completing one.
The nurse should facilitate a power of attorney for health care document only if the client wishes to designate a health care proxy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. The client has a decreased energy level.A decreased energy level can be a common symptom of many conditions, including terminal illnesses. While it can be associated with feelings of hopelessness, it is not necessarily an indication of it. Other factors like the illness itself, treatments, or emotional stress can contribute to low energy.
B. The client requests a second opinion.Requesting a second opinion is generally a sign that the client is still actively engaged in their care and is seeking more information or alternative options. It indicates hope or a desire for different possibilities rather than hopelessness.
C. The client wants to talk about the diagnosis with the nursing staff.Wanting to talk about the diagnosis with the nursing staff suggests that the client is processing the information and seeking support. Open communication is a positive coping mechanism and not typically an indication of hopelessness.
D. The client makes funeral arrangements.When a client makes funeral arrangements, it can be a sign that they are feeling hopeless about their situation and are preparing for the end of their life. While it is practical and sometimes necessary to make such arrangements, in this context, it can be seen as a manifestation of hopelessness.
Correct Answer is D
Explanation
Choice A reason:
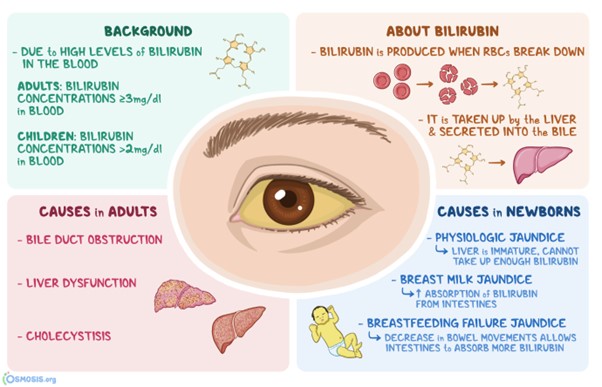
The face is incorrect: Facial skin colour can vary for many reasons, but it may not be the best indicator of jaundice in individuals with dark skin.
Choice B reason
Shoulders is incorrect: The shoulders are not typically indicative of jaundice.
Choice C reason:
Palm of the hands is incorrect: While the palm of the hands can sometimes show yellowing in cases of jaundice, it is less reliable than observing the sclera.
Choice D reason:
Sclera is the best location. In individuals with darker skin tones, yellowish discoloration of the skin due to jaundice can be more challenging to detect. However, the sclera of the eyes can still show noticeable yellowing, making it a reliable location for assessing jaundice in individuals with both light and dark skin.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today