A nurse is assessing a newborn following a vaginal delivery. Which of the following findings should the nurse report to the provider?
Heart rate 136/min
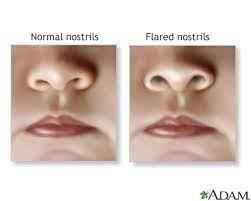
Nasal flaring
Transient strabismus
Overlapping of sutures
The Correct Answer is B
- A. Heart rate 136/min is a normal finding for a newborn. The normal range of heart rate for a newborn is 100 to 160/min.
- B. Nasal flaring is an abnormal finding for a newborn. Nasal flaring indicates respiratory distress and may be caused by conditions such as pneumonia, meconium aspiration, or congenital heart defects.
- C. Transient strabismus is a normal finding for a newborn. Transient strabismus is a temporary misalignment of the eyes that occurs due to weak eye muscles and poor coordination. It usually resolves by 3 to 6 months of age.
- D. Overlapping of sutures is a normal finding for a newborn. Overlapping of sutures is caused by molding of the skull during delivery and allows the head to fit through the birth canal. It usually resolves within a few days after birth.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Hypoxemia is a condition of low oxygen levels in the blood. PEEP can actually improve oxygenation by preventing alveolar collapse and increasing functional residual capacity.
B. Tension pneumothorax is a life-threatening condition of air accumulation in the pleural space that causes increased intrathoracic pressure and compresses the lungs, heart, and great vessels. PEEP can increase the risk of tension pneumothorax by creating excessive positive pressure in the airways and alveoli.
C. Malignant hypertension is a severe form of high blood pressure that can cause organ damage and stroke. PEEP can cause a transient increase in blood pressure due to increased intrathoracic pressure, but it does not cause malignant hypertension.
D. Atelectasis is a condition of partial or complete lung collapse due to alveolar collapse or obstruction. PEEP can prevent or treat atelectasis by maintaining positive pressure in the airways and alveoli.
Correct Answer is A
Explanation
- A. Correct. The nurse should initiate seizure precautions for a client who is at 33 weeks of gestation and has severe gestational hypertension, which is a blood pressure of 160/110 mm Hg or higher on two occasions at least 4 hr apart, or once with signs of end-organ damage. Severe gestational hypertension can lead to preeclampsia, which is a condition characterized by hypertension, proteinuria, and edema, and can progress to eclampsia, which is a lifethreatening complication that involves seizures.
- B. Incorrect. The nurse does not need to initiate seizure precautions for a client who is at 16 weeks of gestation and has a hydatidiform mole, which is an abnormal growth of placental tissue that resembles grape-like clusters. A hydatidiform mole can cause vaginal bleeding, hyperemesis gravidarum, and elevated human chorionic gonadotropin levels, but it does not increase the risk of seizures.
- C. Incorrect. The nurse does not need to initiate seizure precautions for a client who is at 28 weeks of gestation and is experiencing vaginal bleeding, which can have various causes such as placenta previa, placental abruption, or cervical trauma. Vaginal bleeding can indicate a potential hemorrhage, but it does not increase the risk of seizures.
- D. Incorrect. The nurse does not need to initiate seizure precautions for a client who is at 36 weeks of gestation and has a positive group B streptococcal culture, which means that the client has bacteria in their vagina or rectum that can cause infection in the newborn during delivery. A positive group B streptococcal culture requires antibiotic prophylaxis during labor, but it does not increase the risk of seizures.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today