A nurse is assessing a newborn following a circumcision. Which of the following findings should the nurse identify as an indication that the newborn is experiencing pain?
Decreased heart rate
Chin quivering
Pinpoint pupils
Slowed respirations
The Correct Answer is B
A. Decreased heart rate: This is not typically an indication of pain in a newborn. Pain can often lead to an increased heart rate as the body responds to stress or discomfort.
B. Chin quivering: This is a common sign of pain in newborns. When infants experience pain, they may exhibit facial expressions such as quivering of the chin, furrowing of the brow, or grimacing.
C. Pinpoint pupils: Pinpoint pupils are not a typical sign of pain in a newborn. This may be associated with certain medications or conditions affecting the nervous system, but it is not a direct indicator of pain.
D. Slowed respirations: While pain can sometimes cause changes in respiratory patterns, slowed respirations alone may not be a reliable indicator of pain in a newborn. Other signs, such as facial expressions or crying, are often more indicative of pain.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is D. Prolonged labor
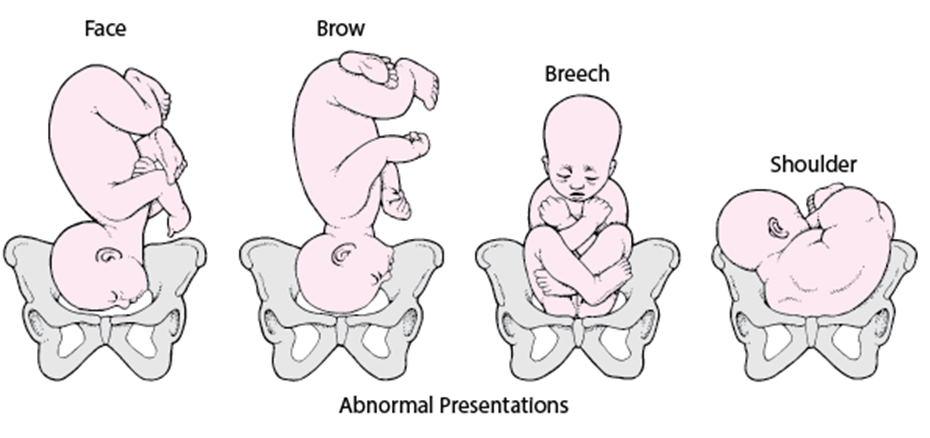
A. Umbilical cord prolapse is more commonly associated with breech presentations or other abnormal fetal positions. It is not a typical complication of occipital brow presentation.
B. Precipitous labor refers to an unusually rapid labor, and it is not a typical complication associated with occipital brow presentation. Prolonged labor is more likely.
C. Hypertonic uterine dysfunction involves excessive uterine contractions, and it is not specifically associated with occipital brow presentation. It is more commonly associated with other factors, such as maternal anxiety or use of oxytocin.
D. Prolonged labor is a complication that can be associated with occipital brow presentation.
Occipital brow presentation involves the fetal head being partially extended, and it can lead to difficulties in descending through the birth canal. This may result in a prolonged labor process.
Correct Answer is C
Explanation
The correct answer is C. Continuous contraction lasting 2 min.
A. Pressure on the perineum causing the client to bear down is a common sign in the later stages of labor when the cervix is fully dilated. It is not typically a cause for immediate concern during the admission phase.
B. Expulsion of clear fluid from the vagina may be amniotic fluid, which can indicate rupture of membranes. While important to note, it is not as urgent as a prolonged contraction.
C. Continuous contraction lasting 2 min is a concerning finding and should be reported first.
A contraction lasting 2 minutes is excessively long and may lead to decreased uterine blood flow, affecting fetal oxygenation. It requires prompt attention from the healthcare provider.
D. Expulsion of a blood-tinged mucous plug, also known as the "bloody show," is a common occurrence in early labor and is not as urgent as the prolonged contraction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today