A nurse is assessing a client who has malnutrition. Which of the following findings should the nurse expect?
Diplopia
Hyperproteinemia
Cachexia
Hypermagnesemia
The Correct Answer is C
Choice A Reason:
Diplopia is incorrect. Diplopia is double vision and is not a specific sign of malnutrition.
Choice B Reason:
Hyperproteinemia is incorrect - Malnutrition often leads to hypoalbuminemia (low levels of albumin, a protein), not hyperproteinemia.
Choice C Reason:
Cachexia is correct. Cachexia refers to a state of severe malnutrition and muscle wasting that can occur in individuals with chronic illnesses, especially advanced cancer, heart failure, or certain inflammatory conditions. It is characterized by significant weight loss, muscle atrophy, weakness, and fatigue. Cachexia goes beyond simple malnutrition and is a more severe manifestation of nutritional deficiency.
Choice D Reason:
Hypermagnesemia is incorrect - Malnutrition is more likely to cause deficiencies in minerals like magnesium, not excess levels (hypermagnesemia).
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Inability to exhale retained carbon dioxide: During an acute asthma attack, airway obstruction due to bronchospasm, inflammation, and increased mucus production leads to air trapping. This makes it difficult for the client to fully exhale, resulting in the retention of carbon dioxide. Hyperinflation of the lungs and respiratory acidosis can occur as a result, contributing to the client's manifestations.
B. Acute loss of alveolar elasticity: A loss of alveolar elasticity is associated with conditions like emphysema, not asthma. Asthma primarily affects the airways rather than the alveoli, and elasticity is not typically impacted during an acute asthma attack.
C. Decreased responsiveness of airways to allergens: Asthma is characterized by increased responsiveness of the airways to triggers such as allergens, not decreased responsiveness. This hyperresponsiveness is a hallmark of the condition and contributes to airway narrowing during an attack.
D. Suppressed bronchiolar inflammatory response: Asthma attacks involve heightened inflammation of the bronchioles, not a suppressed inflammatory response. The inflammation contributes to airway swelling, increased mucus production, and bronchospasm.
Correct Answer is A
Explanation
Choice A reason:
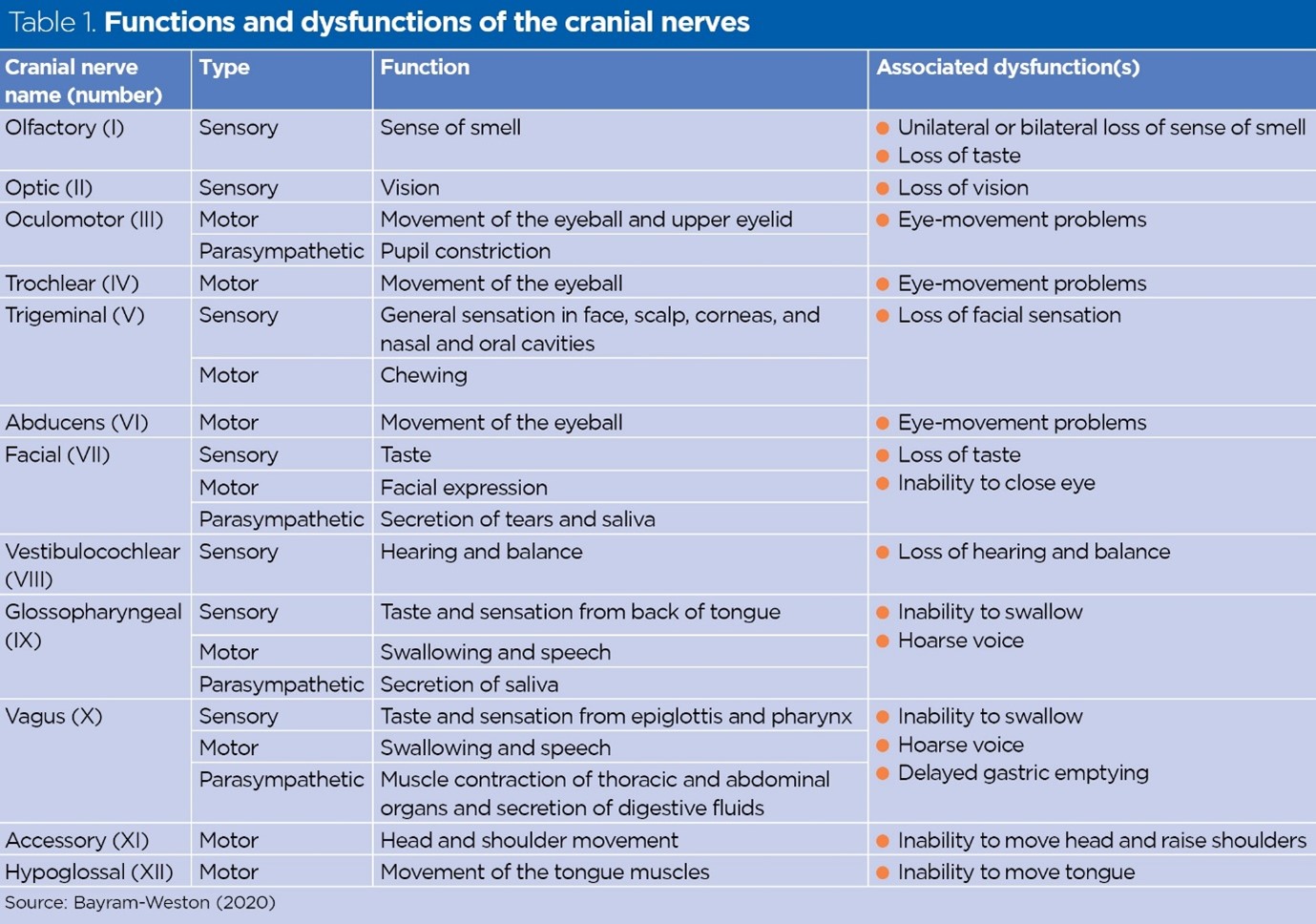
Disequilibrium with movement is correct. The vestibulocochlear nerve (cranial nerve VIII) is responsible for both hearing (cochlear component) and balance (vestibular component). Impaired function of this nerve can result in problems with equilibrium and balance, leading to symptoms such as disequilibrium or vertigo (a sensation of spinning or whirling), especially with movement.
Choice B Reason:
Deviation of the tongue from midline is incorrect. This is related to cranial nerve XII (hypoglossal nerve) and its role in tongue movement and control.
Choice C Reason:
Loss of peripheral vision is incorrect. This is related to cranial nerve II (optic nerve) and its role in vision.
Choice D Reason:
Inability to smell is incorrect. This is related to cranial nerve I (olfactory nerve) and its role in the sense of smell.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today