A nurse is admitting a client who is at 37 weeks of gestation and diagnosed with severe gestational hypertension. Which of the following actions should the nurse expect to implement? (Select all that apply.)
Evaluate neurologic status every 8 hr.
Provide a dark, quiet environment.
Administer magnesium sulfate IV.
Ensure that calcium gluconate is readily available.
Assess respiratory status every 4 hr.
Correct Answer : B,C,D
Explanation:
A. Evaluate neurologic status every 8 hr.
While monitoring neurologic status is important in clients with severe gestational hypertension to assess for signs of impending eclampsia (seizures), more frequent monitoring is typically required, such as every 4 hours or even more frequently depending on the severity of the condition. Therefore, evaluating neurologic status every 8 hours is not sufficient for this client.
B. Provide a dark, quiet environment.
Creating a calm and low-stimulation environment helps to reduce the risk of seizures, which can be triggered by bright lights and loud noises in clients with severe gestational hypertension.
C. Administer magnesium sulfate IV.
Magnesium sulfate is commonly used to prevent seizures in clients with severe gestational hypertension (preeclampsia). It is a standard treatment to prevent eclampsia, a serious complication of preeclampsia characterized by seizures. Therefore, the nurse should expect to administer magnesium sulfate IV as part of the management plan for severe gestational hypertension.
D. Ensure that calcium gluconate is readily available.
Magnesium sulfate, while effective in preventing seizures, can lead to magnesium toxicity if levels become too high. Calcium gluconate is the antidote for magnesium sulfate toxicity. Therefore, the nurse should ensure that calcium gluconate is readily available to counteract any potential magnesium toxicity that may occur during magnesium sulfate administration.
E. Assess respiratory status every 4 hr.
Monitor and record vital signs (blood pressure, pulse, respirations, O2 saturation) every 1 hour x’s 8 hours after maintenance infusion is started and vital signs for bolus infusion are complete. If respiratory rate < 12 breaths/min, draw magnesium level, notify HCP, and observe closely.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Explanation:
A. Slightly below the umbilicus:
Around 16-20 weeks of gestation, the fundal height is typically palpated slightly below the umbilicus. This corresponds to the level of the fundus before it starts rising significantly above the umbilicus as the pregnancy progresses.
B. 3 cm above the umbilicus:
At 22 weeks of gestation, the fundal height is expected to be approximately 3 cm above the umbilicus. This is a common estimation for the fundal height at this stage of pregnancy, as the uterus continues to grow and the fundus ascends in a predictable manner.
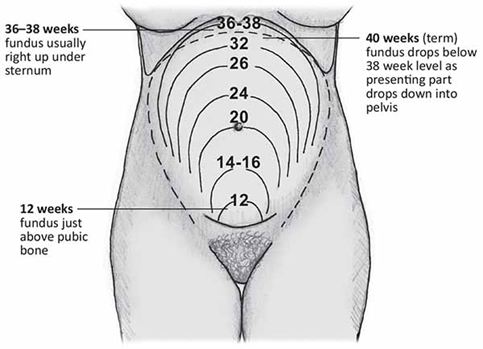
C. 3 cm below the umbilicus:
Palpating the fundus 3 cm below the umbilicus would typically correspond to an earlier gestational age, such as around 16-18 weeks. As pregnancy advances, the fundal height increases, and by 22 weeks, it should be well above the level of the umbilicus.
D. Slightly above the umbilicus:
This location is closer to where the fundal height is expected to be at later gestational ages, such as 24-26 weeks. However, at 22 weeks of gestation, the fundal height should not be palpated slightly above the umbilicus but rather around 3 cm above it.
Correct Answer is C
Explanation
Explanation:
A. Women during labor and birth:
Maternity nursing does involve caring for women during labor and birth. Nurses in labor and delivery units provide support, monitoring, and assistance to women as they progress through labor and deliver their babies. This aspect of maternity nursing focuses specifically on the care of women during the active stages of childbirth, including pain management, labor progression, and ensuring a safe delivery experience.
B. Mothers and fathers during hospitalization for childbirth:
Maternity nursing also involves caring for both mothers and fathers during their hospitalization for childbirth. Nurses provide education, support, and assistance to new parents as they adjust to the postpartum period and learn to care for their newborns. This includes teaching about newborn care, breastfeeding support, postpartum recovery, and emotional support for the entire family unit.
C. Families during the childbearing process:
This choice is the most comprehensive and accurate description of the client focus in maternity nursing. Maternity nursing encompasses care for entire families during the entire childbearing process, from preconception to postpartum. This includes providing education, support, and guidance to expectant parents, assisting with childbirth, promoting bonding and attachment between parents and newborns, and addressing the physical and emotional needs of the family as they navigate the transitions of pregnancy, childbirth, and early parenthood.
D. Childbearing women during acute illness:
While maternity nursing does involve caring for childbearing women during periods of acute illness related to pregnancy or childbirth complications, this focus is more limited compared to the broader scope of caring for families throughout the entire childbearing process. Maternity nurses may be involved in managing complications such as preeclampsia, gestational diabetes, or postpartum hemorrhage, but their role extends beyond acute illness management to include comprehensive prenatal, intrapartum, and postpartum care for women and their families.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today