A nurse is about to administer an intermittent enteral feeding to a client who has an NG tube in place. Besides obtaining an x-ray, which of the following methods should the nurse use to verify the placement?
Inject air and listen for bubbling.
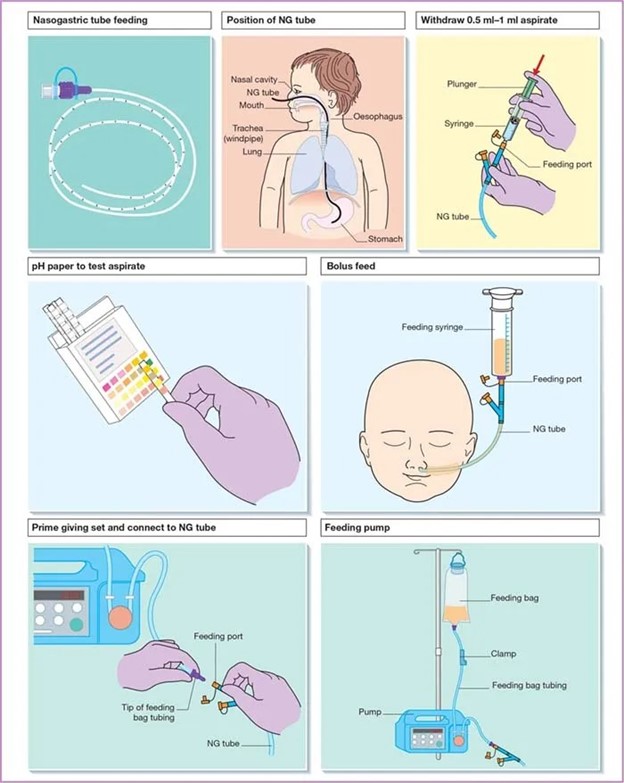
Test the pH of the gastric aspirate.
Measure the gastric residual.
Add food coloring to the formula.
The Correct Answer is B
This is done by aspirating a small amount of stomach contents and testing the pH using pH paper or a pH indicator strip. The pH of stomach contents is typically acidic (pH less than 5), indicating proper placement in the stomach.
Injecting air and listening for bubbling is not a reliable method to verify tube placement, as it can lead to complications such as pneumothorax.
Measuring gastric residual is done to assess the amount of gastric contents remaining in the stomach, but it does not confirm tube placement.
Adding food coloring to the formula is not a standard practice and does not provide reliable confirmation of tube placement.
X-ray is the gold standard method to confirm tube placement but is not typically done before every intermittent feeding unless there are concerns about tube placement
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Explanation:
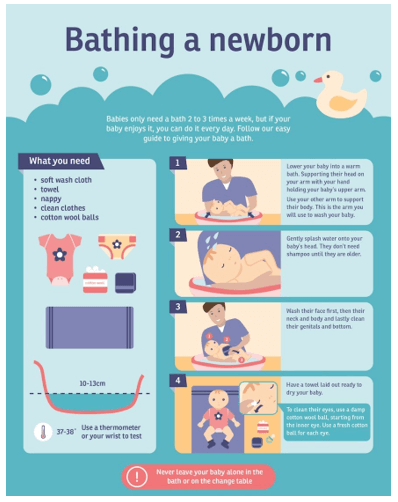
Sponge baths are recommended until the umbilical cord stump falls off, which typically occurs within the first two weeks of life. After that, the baby can be immersed in water for a regular bath.
Using talcum powder is not recommended as it can be harmful to the baby's respiratory system if inhaled. Mild, pH-balanced soap should be used instead of alkaline soap to avoid irritating the baby's delicate skin.
The bathwater temperature should be around 98 degrees Fahrenheit and not hoter than 100 degrees Fahrenheit to prevent burns.
Correct Answer is A
Explanation
a. Clean the stoma using an inward to outward circular motion.
When providing tracheostomy care, the nurse should clean the stoma using an inward to outward circular motion to remove any secretions or debris. It is important to avoid using excessive force or pressure, which can cause trauma to the stoma. Cleansing the inner cannula with isopropyl alcohol may be appropriate for some clients, but it is important to follow the healthcare provider's orders regarding inner cannula care.
When securing the tracheostomy ties, the nurse should ensure that there is enough space for two fingers, not three. Finally, the nurse should prepare sterile supplies before removing the inner cannula to ensure that they are readily available and reduce the risk of infection.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today