A nurse in an emergency department is assessing a client who has experienced a right hemispheric stroke. Which of the following findings should the nurse expect?
Aphasia
Depression
Loss of depth perception
Slow, cautious behavior
The Correct Answer is C
Choice A rationale:
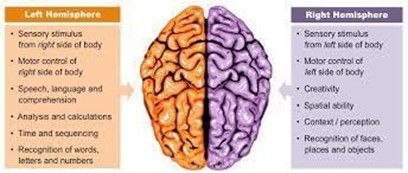
Aphasia, or difficulty with language, is more commonly associated with left hemispheric stroke.
Choice B rationale:
Depression can be a common psychological reaction following stroke, but it is not a specific finding associated with right hemispheric stroke.
Choice C rationale:
Right hemispheric stroke can lead to loss of depth perception and spatial awareness due to its impact on the visual-spatial processing areas of the brain.
Choice D rationale:
Slow, cautious behavior is a common finding after stroke regardless of the affected hemisphere.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
Survivors of sexual assault can exhibit a wide range of psychological symptoms, and their experiences may vary significantly. There is no universal pattern of symptoms that applies to all survivors.
Choice B rationale:
Psychotherapy, such as trauma-focused cognitive-behavioral therapy, has been shown to be effective in helping survivors of sexual assault cope with and heal from their experiences.
Choice C rationale:
Rationale:
It is important to emphasize that sexual assault survivors often know the perpetrator, as this information dispels the myth that most assaults are committed by strangers.
Education should provide accurate and evidence-based information to address misconceptions.
Choice D rationale:
Survivors of sexual assault come from diverse backgrounds and living situations, and their marital status or residence in metropolitan areas is not universally applicable.
Correct Answer is B
Explanation
Choice A rationale:
Frequent cervical examinations may increase the risk of introducing infection or causing additional bleeding. Cervical examinations are not a priority in managing placental abruption.
Choice B rationale:
Placental abruption can lead to significant blood loss, and the client may require intravenous fluids and blood products to maintain hemodynamic stability. Initiating an IV with an 18-gauge catheter allows for rapid administration of fluids and blood products if needed.
Choice C rationale:
Monitoring fetal heart rate hourly is important, but addressing the mother's hemodynamic stability with IV fluids takes priority.
Choice D rationale:
Vital signs should be obtained more frequently than every 4 hours due to the risk of ongoing blood loss.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today