A nurse in an adult day care facility is contributing to the plan of care for a client whose family reports recent confusion and memory loss.
Which of the following strategies should the nurse include in the plan?
Maintain low-level lights in common areas.
Give the client several meal options at lunchtime.
Confront the client regarding inappropriate behavior.
Use symbols in the communal room signage.
The Correct Answer is D
A. Maintain low-level lights in common areas. Low-level lighting can increase confusion and the risk of falls, especially for clients with memory loss. It is important to have adequate lighting to promote a safe environment and help with orientation. Well-lit areas can reduce disorientation and anxiety in clients who are confused or have memory issues.
B. Give the client several meal options at lunchtime. For clients with memory loss and confusion, it is better to provide simple choices or pre-selected meals to reduce decision-making stress and confusion.
C. Confront the client regarding inappropriate behavior. Confronting a client with memory loss or confusion about inappropriate behavior can increase agitation, anxiety, and defensive reactions.
D. Use symbols in the communal room signage. Symbols and pictures can help clients with memory loss navigate their environment more easily because they may have difficulty reading or comprehending written language. Visual cues such as symbols in signage can improve orientation and independence, helping the client feel more comfortable in their surroundings.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
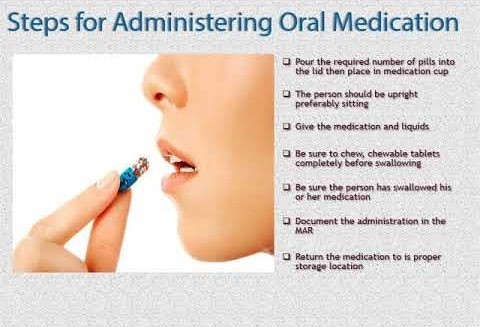
When administering oral medications, the nurse should verify the medication three times with the medication administration record to ensure that the correct medication is being given to the correct client at the correct time. This is known as the "three checks" and is an important step in preventing medication errors.
Correct Answer is D
Explanation
In this scenario, the nurse disclosed sensitive medical information about the client's diagnosis to someone who is not directly involved in the client's care or treatment. This disclosure violates the client's right to privacy and confidentiality.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today