A nurse in a postpartum unit is caring for several clients. After receiving a change-of-shift report, which of the following clients should the nurse assess first?
A client who is 2 days postpartum and whose fundus is 2 fingerbreadths below the umbilicus
A client who is 1 day postpartum and has not voided in 8 hr
A client who is 3 days postpartum and has not had a bowel movement since prior to admission
A client who is 4 days postpartum and has lochia serosa
The Correct Answer is B
A. A fundal height of 2 fingerbreadths below the umbilicus in a client who is 2 days postpartum is within the expected range for that time frame and does not require immediate assessment.
B. A client who is 1 day postpartum and has not voided in 8 hours may be at risk for urinary retention, which can lead to complications such as bladder distension or urinary tract infection. Prompt assessment and intervention are needed.
C. Not having a bowel movement since prior to admission is not an urgent concern in the
immediate postpartum period, especially if the client is otherwise stable and not experiencing discomfort or other symptoms.
D. Lochia serosa, which is the normal vaginal discharge that occurs 3 to 10 days postpartum, is not an urgent concern and does not require immediate assessment.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A.
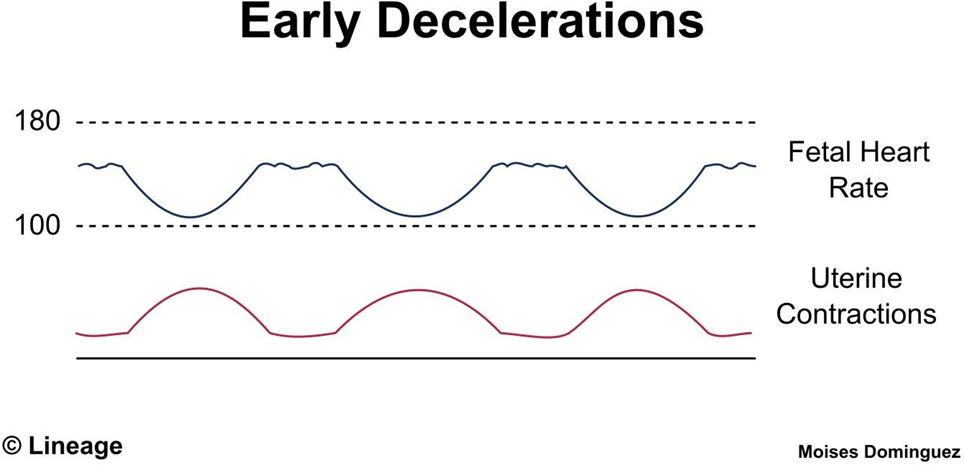
A. Early decelerations are typically benign and occur due to head compression during
contractions. They mirror the uterine contraction pattern and are not usually associated with fetal compromise.
B. Fetal hypoxia is not typically associated with early decelerations, as they are considered a normal response to head compression during labor.
C. Abruptio placentae refers to the premature separation of the placenta from the uterine wall and is not directly related to early decelerations.
D. Postmaturity refers to a pregnancy that extends beyond 42 weeks gestation and is not directly related to early decelerations.
Correct Answer is D
Explanation
A. A blood glucose level of 120 mg/dL is within the expected range for a client receiving total parenteral nutrition and does not require immediate intervention.
B. A serum sodium level of 138 mEq/L is within the normal range and does not require immediate intervention.
C. An oral temperature of 37.6°C (99.7°F) is slightly elevated but may be within the client's normal range and does not require immediate intervention unless accompanied by other signs of infection.
D. A weight increase of 2 kg (4.4 lb) in the past 24 hours indicates fluid overload, which can lead to complications such as heart failure or pulmonary edema. Immediate intervention, such as adjusting the rate of fluid administration or notifying the healthcare provider, is necessary to prevent further complications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today