A nurse enters a client’s room to answer the call light and finds the client on the bathroom floor. What should be the nurse’s initial action?
Assist the client back into bed.
Notify the client’s provider.
Inform the client’s family member.
Obtain the client’s vital signs.
The Correct Answer is D
The correct answer is choice D.
Choice A rationale:
Assisting the client back into bed is not the initial action. Moving the client without assessing their condition could potentially cause harm.
Choice B rationale:
Notifying the client’s provider is important, but it should be done after assessing the client’s condition to provide accurate information.
Choice C rationale:
Informing the client’s family member is not the immediate priority. The nurse should first ensure the client’s safety and assess their condition.
Choice D rationale:
Obtaining the client’s vital signs is the initial action. This helps assess the client’s current condition and determine if there are any immediate medical needs.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale:
The spinal cord plays a crucial role in pain transmission, but it does not initiate the afferent pathways. It receives pain signals from nociceptors and relays them to the brain for processing.
The spinal cord is also involved in pain modulation, as it can dampen or amplify pain signals depending on various factors. However, it is not the primary trigger for pain sensation. That role belongs to nociceptors.
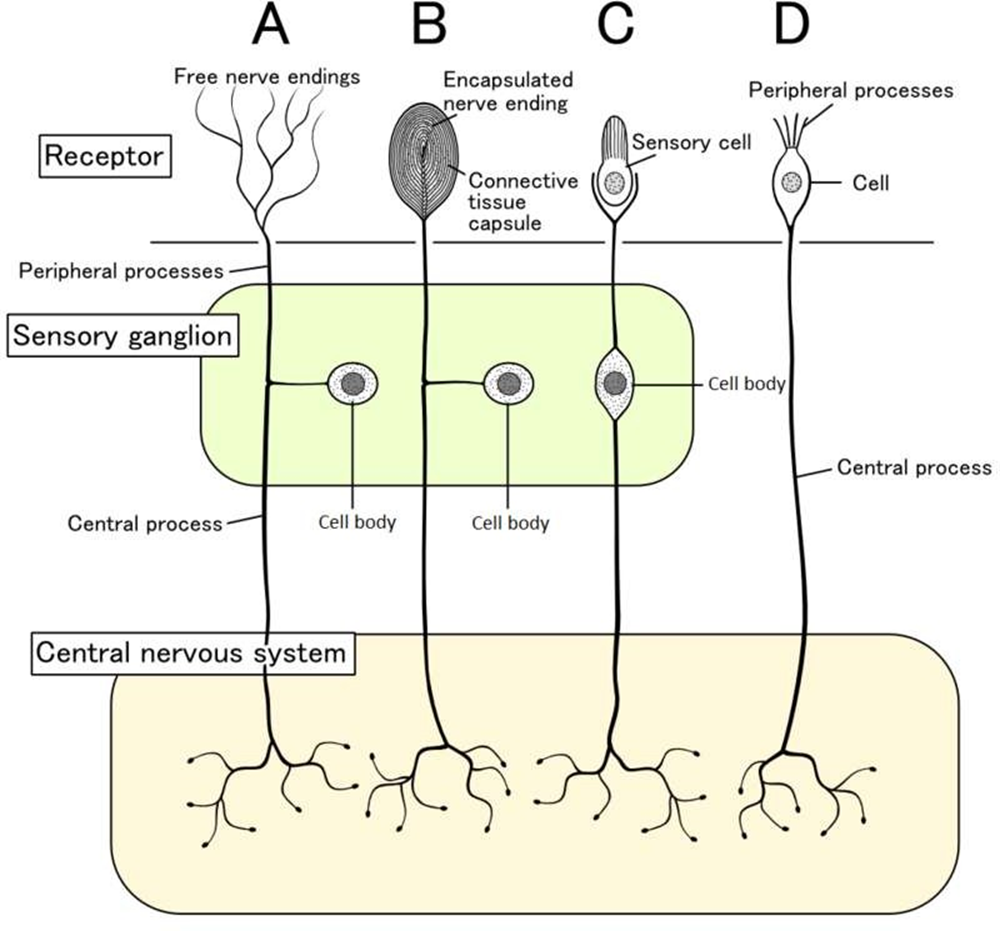
Choice B rationale:
Nociceptors are specialized sensory receptors that detect potentially damaging stimuli, such as intense heat, pressure, or chemical irritants.
They are located throughout the body, including the skin, muscles, joints, and internal organs.
When nociceptors are activated, they generate electrical signals that travel along nerve fibers to the spinal cord and brain. This process initiates the afferent pathways, which ultimately lead to the conscious perception of pain.
Nociceptors are essential for protecting the body from harm. They alert us to potential dangers and trigger responses that help us avoid injury or further damage.
Choice C rationale:
Endorphins are natural pain-relieving substances produced by the body. They act on receptors in the brain and spinal cord to reduce pain perception.
However, endorphins do not trigger the afferent pathways. They work by modulating pain signals that have already been initiated by nociceptors.
Choice D rationale:
The cortex is the outer layer of the brain that is responsible for higher-level functions, such as thinking, feeling, and decision- making.
It plays a role in the conscious experience of pain, but it does not trigger the afferent pathways.
The cortex receives pain signals from the spinal cord and processes them, leading to the awareness of pain.
Correct Answer is A
Explanation
The correct answer is Choice A.
Choice A rationale: Encouraging increased fluid intake helps maintain blood volume and reduces viscosity, promoting circulation and lowering the risk of venous stasis and clot formation postoperatively.
Choice B rationale: Keeping the affected knee flexed impairs venous return and increases stasis, elevating the risk of thrombosis. Proper positioning with extension promotes circulation and reduces clot risk.
Choice C rationale: Prolonged bed rest contributes to immobility-induced venous stasis, a major risk factor for DVT. Early ambulation and leg exercises are essential to prevent thromboembolic events.
Choice D rationale: Massaging the calf of a postoperative patient is contraindicated due to the risk of dislodging a thrombus, potentially leading to a life-threatening pulmonary embolism.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today