A male client with a chronic medical condition tells the practical nurse (PN) that he wants no heroics to prolong his life if anything should happen to him. Which action should the PN take?
Place a "Do Not Resuscitate" sign outside the client's door and at the bedside.
Reassure the client that life-saving measures will not be taken without consent.
Complete an advance directive form and place it in the medical record.
Notify the client's healthcare provider of the client's wishes as soon as possible.
The Correct Answer is D
A. "Place a 'Do Not Resuscitate' sign outside the client's door and at the bedside."
A DNR order must be written by the healthcare provider and documented in the medical record. A sign alone is not sufficient to ensure the client’s wishes are followed.
B. "Reassure the client that life-saving measures will not be taken without consent."
While reassuring the client is important, the client’s wishes must be documented formally through an advance directive, which is legally binding and ensures that medical staff are aware of and follow the client’s instructions.
C. "Complete an advance directive form and place it in the medical record."
While completing an advance directive is important, the first priority is notifying the healthcare provider so that the client’s wishes can be documented and the proper legal forms can be completed.
D. "Notify the client's healthcare provider of the client's wishes as soon as possible."
The nurse should immediately notify the healthcare provider of the client’s wishes. The healthcare provider can then initiate the appropriate legal documentation, such as a DNR order or an advance directive, ensuring the client’s wishes are respected in the future. This is the first step in ensuring that the client’s preferences are followed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Gently blowing the nose helps to clear any mucus or debris from the nasal passages, allowing for better delivery and absorption of the medication. It also helps to ensure that the nasal passages are clear and open, allowing the medication to reach its intended target.
A. Deep breathing and coughing are unrelated to the administration of nasal spray and are not necessary before using the medication.
B. Checking glucose levels before and after administration is not relevant for fluticasone furoate nasal spray. Glucocorticoid nasal sprays are not typically associated with significant effects on blood glucose levels.
C. Exhaling through the mouth is not a specific action required before using the nasal spray. It may be a general instruction for some other respiratory therapies or procedures, but it is not directly related to the administration of the nasal spray.
Correct Answer is D
Explanation
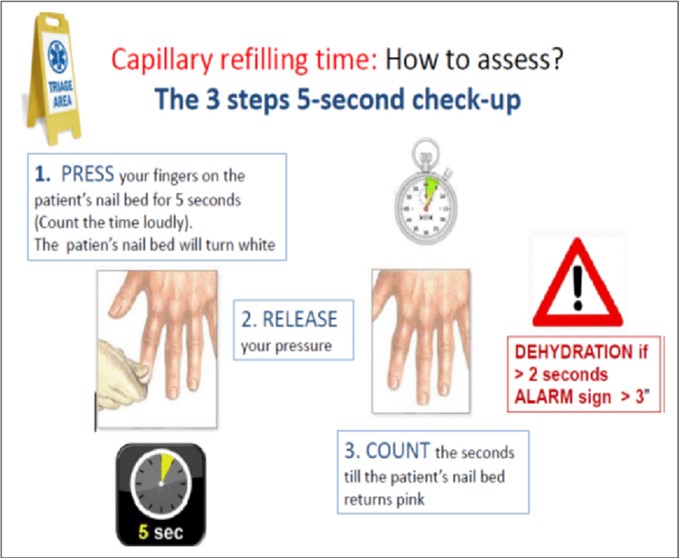
- Capillary refill time is a test that measures how quickly the blood returns to the tissues after pressure is applied and released on a nailbed or a fingertip. It is an indicator of peripheral circulation and tissue perfusion.
- To perform the capillary refill test, the examiner should press firmly on the nailbed or fingertip for a few seconds, then release the pressure and observe how long it takes for the normal color to return. The normal capillary refill time is less than 2 seconds .
- In the photo, the practical nurse (PN) applies and then releases pressure to a client's fingernail. Normal nail color returns in 2 seconds, which indicates a normal capillary refill time and adequate peripheral circulation. This is a normal and expected finding that does not require any further action, except for documentation.
- Therefore, option D is the correct answer, as it reflects the appropriate and standard nursing practice of documenting any assessment findings in the client's chart. Option D also implies that the PN does not need to report, observe, or repeat anything else related to the capillary refill test, as it was done correctly and yielded normal results.
- Options A, B, and C are incorrect answers, as they do not reflect the appropriate or necessary actions for the PN to take after performing a normal capillary refill test.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today