A homeless client arrives in the emergency room. The client verbalizes an inability to bathe for at least one month. What is the nurse's priority?
Inspect the client's skin
Provide a towel and show the client to the shower
Ask if the client has been to a homeless shelter recently
Call a social worker
The Correct Answer is A
Choice A reason: Inspecting the client's skin is the nurse's priority, because it is the most urgent and relevant action. Inspecting the client's skin can help identify any signs of infection, injury, or infestation, such as wounds, rashes, ulcers, or lice. The client's skin may be compromised by the lack of hygiene, exposure to the elements, or poor nutrition. The client's skin may also be a source of transmission of pathogens to other clients or staff. Therefore, inspecting the client's skin is essential for the assessment, diagnosis, and treatment of the client's condition.
Choice B reason: Providing a towel and showing the client to the shower is not the nurse's priority, because it is not the most urgent and relevant action. Providing a towel and showing the client to the shower is an important intervention, but it should be done after inspecting the client's skin and ensuring the safety and infection prevention of the client and others. The client may have wounds, rashes, or ulcers that need to be cleaned, dressed, or treated before bathing. The client may also have lice or scabies that need to be isolated and treated with special shampoos or creams before bathing. The client may also need assistance or supervision during bathing, depending on the client's physical and mental status.
Choice C reason: Asking if the client has been to a homeless shelter recently is not the nurse's priority, because it is not the most urgent and relevant action. Asking if the client has been to a homeless shelter recently is an important question, but it should be done after inspecting the client's skin and providing a towel and showing the client to the shower. The client's history of homelessness and shelter use may provide some information about the client's social and environmental factors, such as exposure to violence, abuse, or disease, or access to resources, services, or support. However, this information is not as critical as the client's skin condition, which may require immediate attention and care.
Choice D reason: Calling a social worker is not the nurse's priority, because it is not the most urgent and relevant action. Calling a social worker is an important referral, but it should be done after inspecting the client's skin, providing a towel and showing the client to the shower, and asking if the client has been to a homeless shelter recently. The social worker can help the client with the psychosocial and practical aspects of homelessness, such as finding a shelter, applying for benefits, accessing health care, or addressing mental health or substance abuse issues. However, this referral is not as urgent as the client's skin condition, which may require immediate attention and care.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
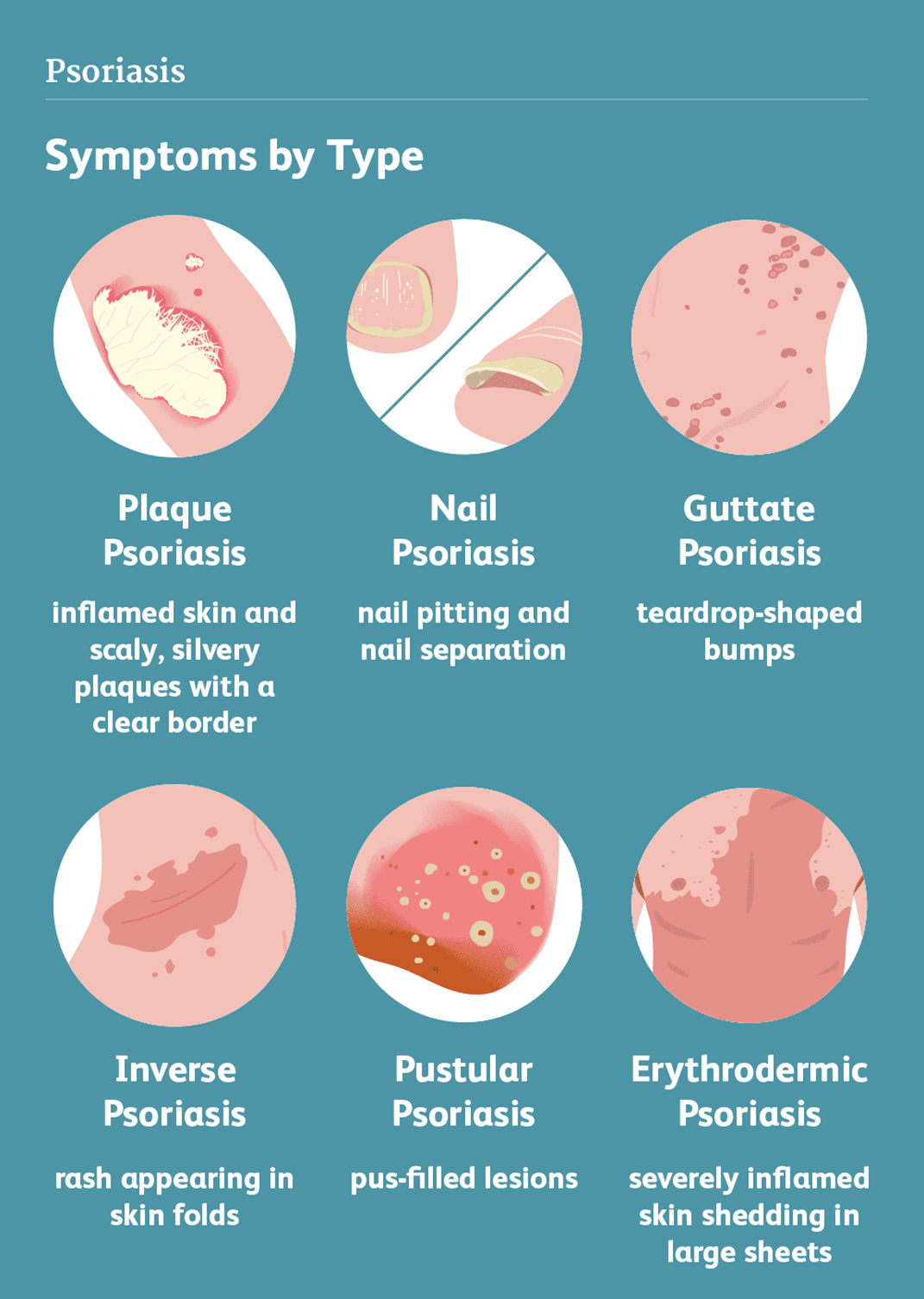
Choice A reason: Psoriasis is a skin abnormality that causes patches of thick, red skin with silvery scales, usually on the elbows, knees, scalp, lower back, or genitals. Psoriasis is a chronic, inflammatory, autoimmune condition that affects the life cycle of skin cells, causing them to build up rapidly on the surface of the skin. Psoriasis can cause itching, burning, pain, or bleeding.
Choice B reason: Rosacea is a skin abnormality that causes redness, flushing, swelling, or pimples, usually on the face, especially the cheeks, nose, chin, or forehead. Rosacea is a chronic, inflammatory, vascular condition that affects the blood vessels and sebaceous glands of the skin. Rosacea can cause sensitivity, stinging, or dryness.
Choice C reason: Scabies is a skin abnormality that causes small, red bumps, blisters, or burrows, usually on the hands, wrists, feet, ankles, or genitals. Scabies is a contagious, parasitic infection that is caused by tiny mites that burrow into the skin and lay eggs. Scabies can cause intense itching, especially at night.
Choice D reason: Stasis dermatitis is a skin abnormality that causes swelling, redness, scaling, or ulcers, usually on the lower legs or ankles. Stasis dermatitis is a chronic, inflammatory condition that results from poor blood circulation in the veins of the legs, causing fluid to leak into the surrounding tissues. Stasis dermatitis can cause pain, itching, or infection.
Correct Answer is A
Explanation
Choice A reason: This is the best intervention because it helps the nurse to understand the client's emotional, social, and practical needs and resources. A new diagnosis of HIV can be a devastating and overwhelming experience for the client, who may face stigma, discrimination, isolation, or rejection from others. The nurse should assess the client's support system, such as family, friends, or community groups, that can provide comfort, guidance, and assistance to the client. The nurse should also encourage the client to seek professional counseling, peer support, or other services as needed.
Choice B reason: This is not the best intervention because it may not respect the client's preferences, beliefs, or values. The nurse should not assume that the client wants or needs spiritual or religious support, unless the client expresses such a desire. The nurse should ask the client about their spiritual or religious beliefs and practices and provide appropriate referrals or resources as requested by the client. The nurse should also respect the client's right to privacy and confidentiality and not disclose the client's diagnosis to anyone without the client's consent.
Choice C reason: This is not the best intervention because it may not be the most urgent or appropriate topic to discuss with the client at this time. The nurse should not focus on the legal or ethical aspects of the client's diagnosis, but rather on the client's emotional and physical wellbeing. The nurse should explain the legal requirement to tell sex partners in a sensitive and respectful manner, but only after the client has accepted and understood their diagnosis and has expressed readiness to disclose their status to others. The nurse should also provide the client with information and resources on how to prevent the transmission of HIV and how to protect themselves and their partners.
Choice D reason: This is not the best intervention because it may not be the client's wish or choice. The nurse should not offer to tell the family for the client, unless the client asks for such help. The nurse should respect the client's autonomy and decisionmaking regarding whom to tell and when to tell about their diagnosis. The nurse should also support the client in preparing for the possible reactions and outcomes of disclosing their status to their family and others.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today