A home health nurse drives up to the house of her client, who has schizophrenia with manic episodes. The client is sitting on his front porch with a shotgun in his arms. Which of the following actions should the nurse take?
Stop the car in the client's driveway and call the authorities.
Honk the car horn to get the client's attention.
Calmly speak the client's name out of the car window.
Keep driving in a path that is going away from the client's house.
The Correct Answer is D
Choice A reason:
Stop the car in the client’s driveway and call the authorities. This statement is wrong because stopping in the driveway could escalate the situation and put the nurse in immediate danger. The nurse should avoid any actions that might provoke the client or put herself in harm’s way.
Choice B reason:
Honk the car horn to get the client’s attention. This statement is wrong because honking the horn could startle the client, potentially leading to a violent reaction. Sudden loud noises can exacerbate agitation in individuals with schizophrenia.
Choice C reason:
Calmly speak the client’s name out of the car window. This statement is wrong because engaging with the client directly while they are armed is unsafe and could provoke aggression. The nurse should avoid direct interaction until the situation is secured.
Choice D reason:
Keep driving in a path that is going away from the client’s house. This is the correct action as it ensures the nurse’s safety by distancing herself from the potentially dangerous situation. Once at a safe distance, the nurse can contact the authorities for assistance.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason:
Acute dystonia is characterized by sudden muscle contractions that can cause abnormal postures. While it is an adverse effect of antipsychotic medications, the symptoms typically include muscle spasms, stiffness, and oculogyric crisis, but not necessarily fever and diaphoresis.
Choice B reason:
Tardive dyskinesia is a late-onset movement disorder associated with prolonged use of antipsychotic medications. It presents with repetitive, involuntary, and purposeless movements, such as grimacing, tongue movements, and lip smacking. Fever and blood pressure changes are not typical features of tardive dyskinesia.
Choice C reason:
Pseudoparkinsonism is an adverse effect of antipsychotic medications that mimics the symptoms of Parkinson's disease, such as tremor, rigidity, bradykinesia, and postural instability. However, it does not usually present with fever or diaphoresis.
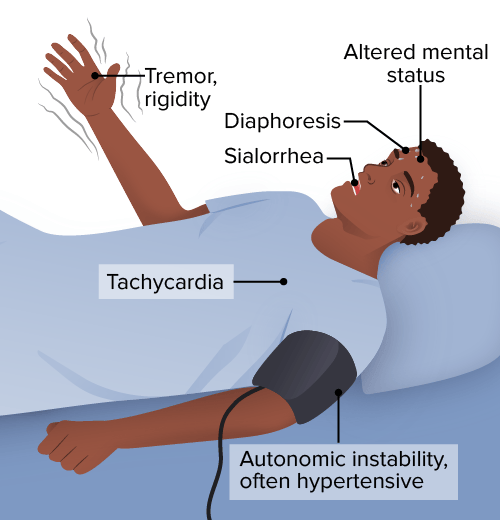
Choice D reason:
Neuroleptic malignant syndrome (NMS) is a life-threatening neurologic emergency associated with the use of antipsychotic medications. It is characterized by mental status changes, muscle rigidity, fever, and autonomic dysfunction, such as blood pressure changes and diaphoresis. NMS requires immediate medical attention and discontinuation of the offending agent.
Correct Answer is ["B","C","D","E"]
Explanation
Choice A Reason:
Schizophrenia cannot be cured with antidepressants. Antidepressants may be used to treat comorbid depression in individuals with schizophrenia, but they do not address the core symptoms of schizophrenia itself. Schizophrenia is a chronic condition that typically requires lifelong treatment with antipsychotic medications to manage symptoms.
Choice B Reason:
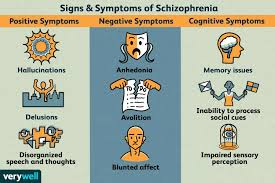
Schizophrenia typically first presents in adolescence or early adulthood. This is the period when symptoms such as hallucinations, delusions, and disorganized thinking often first become apparent. The onset of schizophrenia during this developmental stage can significantly impact an individual's social and vocational abilities.
Choice C Reason:
Antipsychotic medications are the cornerstone of schizophrenia treatment. They can be used to manage symptoms of hallucinations and delusions, which are known as positive symptoms of schizophrenia. These medications work by affecting neurotransmitters in the brain, particularly dopamine.
Choice D Reason:
Individuals with schizophrenia have a higher risk of substance abuse disorders. Substance use can exacerbate symptoms of schizophrenia and complicate the course of the illness. It is important for treatment plans to address any co-occurring substance use disorders.
Choice E Reason:
Schizophrenia significantly affects thoughts and perceptions. It can cause distorted thinking patterns, false beliefs, and sensory experiences that others do not share. These symptoms can be distressing and may lead to difficulties in distinguishing reality.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today