A client with newly diagnosed Crohn's disease asks the nurse about dietary restrictions. How should the nurse respond?
Instruct the client to avoid foods with gluten, such as wheat bread.
Explain that the need to restrict fluids is the primary limitation.
Advise the client to limit foods that are high in calcium and iron.
Describe the use of an elimination diet to find trigger foods
The Correct Answer is D
A. Instruct the client to avoid foods with gluten, such as wheat bread.
While some individuals with Crohn's disease may experience improvement by avoiding certain types of carbohydrates, including gluten, this recommendation is not universally applicable to all individuals with Crohn's disease. Gluten restriction is more relevant for those with gluten sensitivity or celiac disease.
B. Explain that the need to restrict fluids is the primary limitation.
This statement is not accurate. Fluid restriction is not a primary dietary limitation for individuals with Crohn's disease. In fact, maintaining adequate hydration is generally important for overall health. Restricting fluids is not a standard dietary recommendation for managing Crohn's disease.
C. Advise the client to limit foods that are high in calcium and iron.
Limiting foods high in calcium and iron is not a standard recommendation for Crohn's disease. In fact, adequate intake of essential nutrients, including calcium and iron, is important for overall health. Limiting these nutrients could lead to nutritional deficiencies.
D. Describe the use of an elimination diet to find trigger foods.
This is the most appropriate response. Crohn's disease symptoms can vary among individuals, and identifying trigger foods through an elimination diet can help personalize dietary recommendations. By systematically eliminating and reintroducing foods, individuals can identify which specific foods may exacerbate their symptoms.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
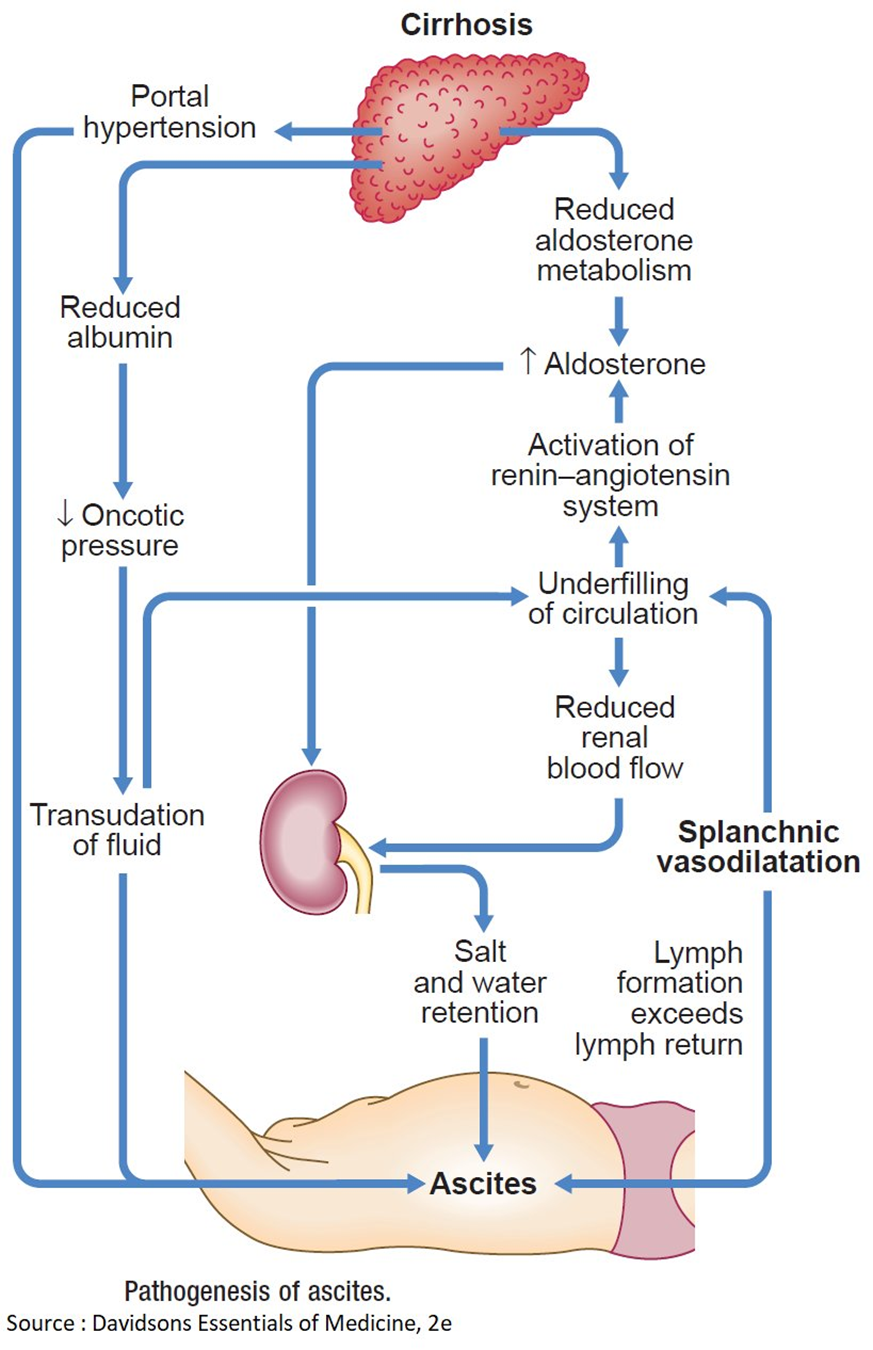
A. Hyperaldosteronism causing an increased sodium reabsorption in renal tubules.
Hyperaldosteronism is characterized by an excess of aldosterone, a hormone that regulates sodium and water balance. In cirrhosis, however, sodium retention is often related to other mechanisms such as portal hypertension and hypoalbuminemia, rather than hyperaldosteronism.
B. Decreased renin-angiotensin response related to an increase in renal blood flow.
Cirrhosis is more commonly associated with an activated renin-angiotensin-aldosterone system, leading to increased sodium and water retention. The increased renin-angiotensin response is a compensatory mechanism to maintain perfusion in the setting of cirrhosis and does not contribute to decreased renal blood flow.
C. Decreased portacaval pressure with greater collateral circulation.
This statement is not accurate. In cirrhosis, there is typically increased portacaval pressure due to portal hypertension, which can lead to the development of collateral circulation. However, this does not explain the edema and ascites seen in cirrhosis.
D. Hypoalbuminemia that results in a decreased colloidal oncotic pressure.
This is the correct choice. In cirrhosis, liver damage leads to decreased synthesis of albumin. Albumin plays a crucial role in maintaining colloidal oncotic pressure, and when it is decreased (hypoalbuminemia), fluid is more likely to leak out of blood vessels, resulting in edema. The same mechanism contributes to the development of ascites in the abdominal cavity.
Correct Answer is D
Explanation
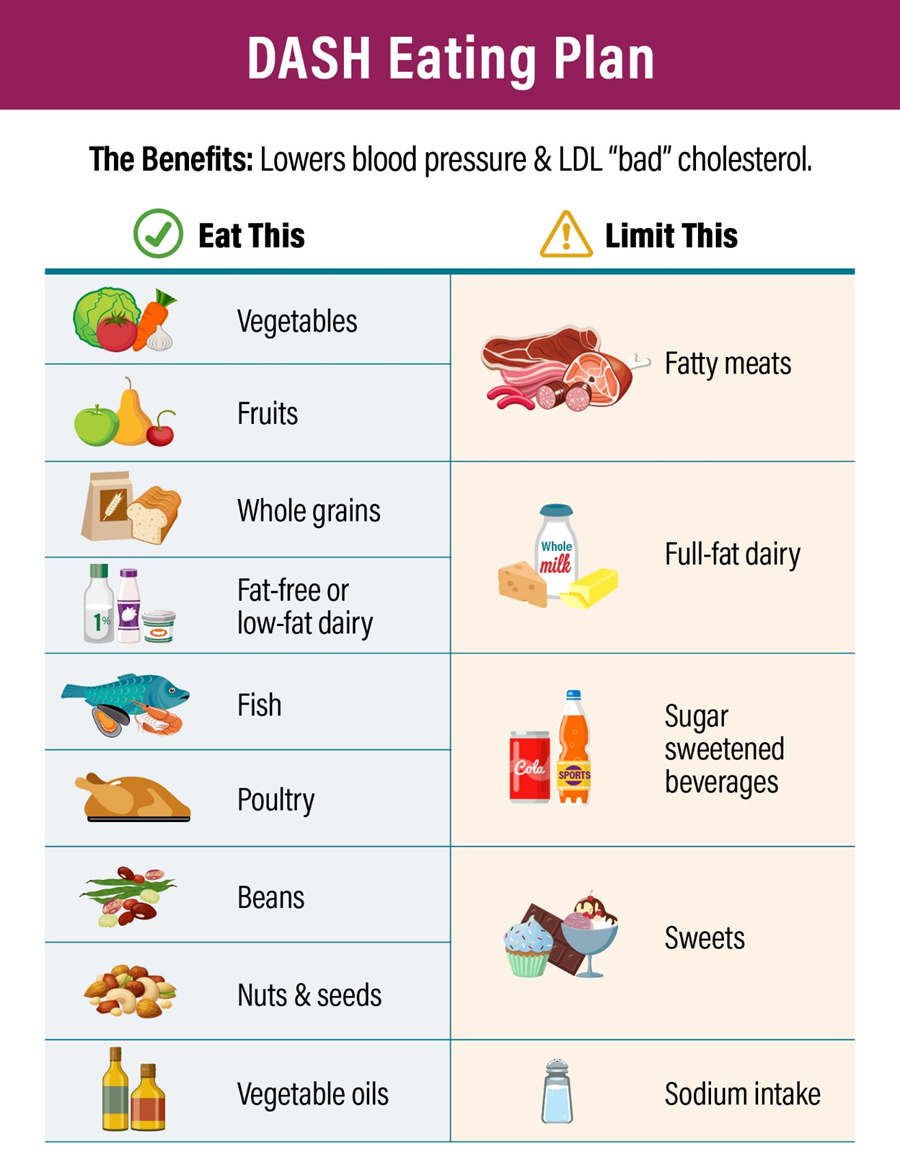
A. Carefully cleans and peels all fresh fruit and vegetables:
While cleaning and peeling fresh fruits and vegetables may contribute to food safety, it is not a specific indication of adherence to the DASH eating plan.
B. Uses only lactose-free dairy products:
The DASH eating plan encourages the consumption of low-fat or fat-free dairy products. Using lactose-free dairy products may be necessary for individuals with lactose intolerance, but it is not a specific behavior related to the DASH plan.
C. No longer includes grains in the daily diet:
The DASH eating plan includes whole grains as part of a balanced diet. Eliminating grains altogether is not consistent with the DASH plan, which encourages the consumption of whole grains.
D. Enjoys fat-free yogurt as an occasional snack food:
This is the correct answer. The DASH eating plan recommends the inclusion of low-fat or fat-free dairy products as part of a heart-healthy diet. Choosing fat-free yogurt as an occasional snack aligns with the principles of the DASH plan, which emphasizes low-fat dairy options.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today