A client with diabetic ketoacidosis (DKA) is receiving regular insulin. Which action should the practical nurse (PN) implement to evaluate the effectiveness of the insulin dosage?
Smell the client's breath for resolution of a fruity odor.
Determine the client's orientation to time and space.
Measure the client's urinary output for an increased volume.
Check fingerstick blood glucose for a decrease in the level.
The Correct Answer is D
Regular insulin is the medication of choice for treating DKA. Its main action is to lower blood glucose levels by promoting the uptake of glucose into cells and inhibiting the production of glucose by the liver. Therefore, checking the fingerstick blood glucose level is an important indicator of the effectiveness of the insulin treatment.
A decrease in the blood glucose level indicates that the insulin is working to lower the high blood sugar associated with DKA. This measurement helps the PN assess the response to treatment and adjust the insulin dosage if necessary.
The other actions mentioned are also important assessments in the care of a client with DKA, but they do not specifically evaluate the effectiveness of the insulin dosage:
A. Smelling the client's breath for resolution of a fruity odor is important as it indicates a decrease in ketone production, which is a marker of improving DKA. However, it does not directly evaluate the effectiveness of the insulin dosage.
B. Determining the client's orientation to time and space is part of assessing their neurological status, which is crucial in managing DKA. However, it does not specifically assess the effectiveness of the insulin dosage.
C. Measuring the client's urinary output for an increased volume is important to monitor hydration status and renal function, but it does not directly evaluate the effectiveness of the insulin dosage.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
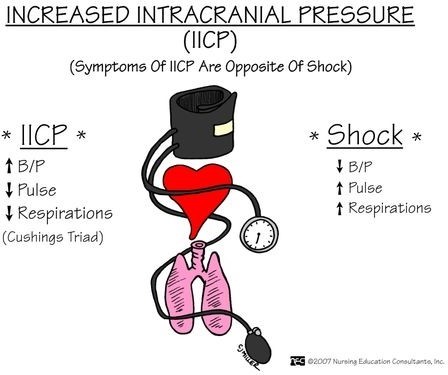
The vital sign trends that indicate increased intracranial pressure (ICP) and should be reported to the charge nurse are:
Bradycardia: A slow heart rate can be a sign of increased ICP.
Irregular respiratory patterns: Abnormal breathing patterns, such as irregular or Cheyne-Stokes respirations, can be indicative of increased ICP.
Widening pulse pressure: An increased difference between systolic and diastolic blood pressure (widening pulse pressure) can be a sign of increased ICP.
A- Heart rate above 110 beats/minute, elevated respiratory rate, and hypotension: While an elevated heart rate and respiratory rate can be associated with increased ICP, hypotension (low blood pressure) is not typically seen in this condition. Hypotension can be a sign of other factors, such as hypovolemia or shock, which may or may not be related to the head injury.
B- Bounding pulse rate, groaning respiratory effort, and elevated blood pressure: Bounding pulse rate and elevated blood pressure are not specific to increased ICP. They can be influenced by other factors such as pain, anxiety, or medications. Groaning respiratory effort may indicate respiratory distress, but it is not directly related to increased ICP.
C- Thready rapid pulse, trembling, perspiration, weakness, and irritability: These signs and symptoms can be associated with various conditions such as anxiety, stress, or other physiological responses. While they may occur in the context of increased ICP, they are not specific to this condition alone.
Correct Answer is A
Explanation
A. Checking the child’s blood glucose level via fingerstick is the most important step before administering insulin to prevent hypoglycemia or ensure the appropriate dose.
B. Exercise affects blood sugar, but the immediate priority is verifying the blood glucose level.
C. Urination patterns can indicate hyperglycemia, but they are not the most critical factor before insulin administration.
D. Eating is important, but insulin dosing should be based on blood glucose readings and meal intake combined.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today