A client whose first child was delivered by cesarean section is 20 weeks pregnant with her second child and wishes to have a vaginal birth after cesarean (VBAC). What information is most important for the practical nurse (PN) to obtain?
Client's intent regarding breastfeeding of the newborn.
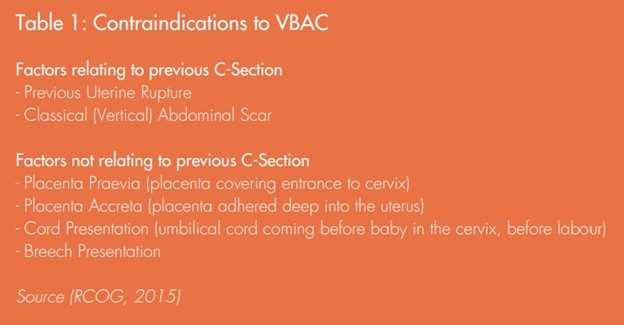
The type of uterine incision used for previous birth.
History of contracting Herpes simplex virus.
Religious preference of the client's family.
The Correct Answer is B
Knowing the type of uterine incision from the previous cesarean section is crucial when considering the option of vaginal birth after cesarean (VBAC). The type of incision can provide important insights into the potential risks and complications associated with a trial of labor.
Specifically, a low transverse uterine incision is considered the most favorable for VBAC, as it has a lower risk of uterine rupture compared to other types of incisions, such as a classical or vertical incision.
A. While information about the client's intent regarding breastfeeding of the newborn is important for providing appropriate support and education, it does not have a direct impact on the decision-making process for VBAC.
C. A history of contracting Herpes simplex virus is relevant to the client's overall health and may have implications for the management of the pregnancy, but it is not directly related to the decision regarding VBAC.
D. The religious preference of the client's family, while important for respecting cultural and spiritual beliefs, does not have a direct impact on the decision-making process for VBAC.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
This comment by the practical nurse (PN) is likely to be the most helpful to the client. By offering to sit with the client, the PN shows empathy, support, and a willingness to provide companionship. This approach acknowledges the client's feelings of isolation and offers a listening ear. It provides an opportunity for the client to express his emotions, thoughts, or concerns if he wishes to do so. The presence of a caring and compassionate individual can help alleviate some of the client's feelings of loneliness and may encourage him to open up and engage in conversation or activities when he is ready.
A. "Come into the recreation area. We have your favorite card game and I will play it with you."
This choice assumes that engaging in a specific activity will automatically help the client and solve his current feelings of reclusiveness. While offering an activity may be beneficial in some cases, it is important to first address the client's emotional state and provide support before suggesting specific activities. Pushing the client to participate in an activity without acknowledging his current feelings may further alienate him and not address the underlying issues causing his reclusive behavior.
B. "Why do you want to stay in your room today?"
This choice may come across as confrontational or judgmental. Asking why the client wants to stay in his room implies that there is something wrong with his decision or that he needs to justify his behavior. This approach may make the client defensive or withdraw further. It is essential to create a safe and supportive environment where the client feels understood and validated, rather than questioning his choices.
C. "I know you are sad about not seeing your family as often, but they are visiting as much as they can."
While acknowledging the client's sadness about not seeing his family is important, dismissing his feelings by stating that his family is visiting as much as they can minimize or invalidate his emotions. It is crucial to provide empathy and validate the client's emotions without making assumptions or downplaying his experiences. This approach may not address the client's current state of reclusiveness or provide the support he needs.
Correct Answer is C
Explanation
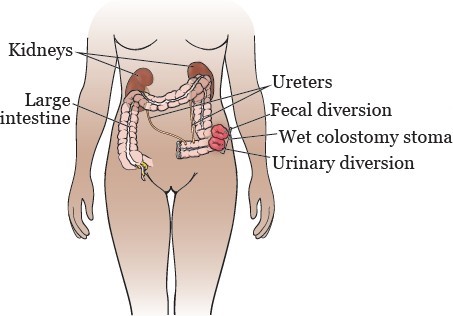
The client's question about whether the surgical opening will be visible suggests that they have concerns or misconceptions about the upcoming fecal diversion surgery. By reviewing the client's expectations of elimination after surgery, the PN can provide accurate information and address any anxieties or concerns the client may have.
The other options are not directly related to the client's question and are not the most appropriate actions to take in this situation:
A. Determining if this is the client's first indwelling catheter is unrelated to the client's question about the visibility of the surgical opening. It may be important to assess the client's history of urinary catheter use for other purposes, but it does not address the client's immediate concern.
B. Asking the client if they finished the bowel sterilization prescription is also unrelated to the visibility of the surgical opening. While bowel sterilization may be a part of the preoperative preparation for fecal diversion surgery, it does not address the client's questions and concerns.
D. Verifying that the client had nothing by mouth (NPO) for the past 24 hours is important for general preoperative care but does not address the client's specific question about the visibility of the surgical opening.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today