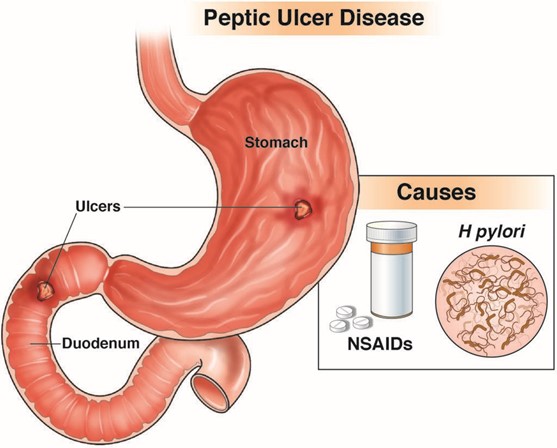
A client was admitted in the hospital with peptic ulcer disease tells the nurse about having black tarry stools. Which of the following is the most appropriate nursing action?
Instruct the client to increase fluid intake.
Notify the health care provider.
Advise the client to take iron rich foods.
Document the findings.
The Correct Answer is B
Choice A Reason: Instructing the client to increase fluid intake is not the most appropriate nursing action, as it does not address the cause or severity of the bleeding.
Choice B Reason: Notifying the health care provider is the most appropriate nursing action, as it indicates that the client may have a bleeding ulcer that requires immediate evaluation and treatment.
Choice C Reason: Advising the client to take iron rich foods is not the most appropriate nursing action, as it does not prevent or correct anemia or bleeding.
Choice D Reason: Documenting the findings is not the most appropriate nursing action, as it does not initiate any intervention or outcome.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
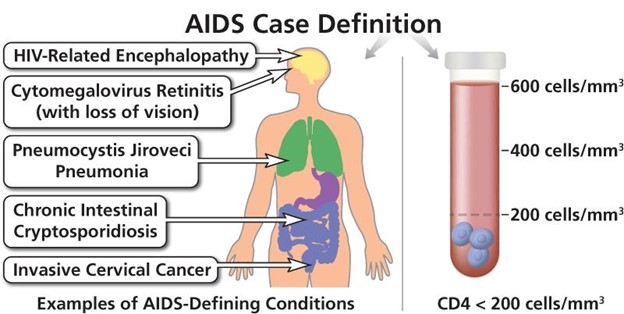
Choice A Reason: Instituting measures to prevent infection is the highest priority in providing care to this client, as AIDS impairs the immune system and makes the client susceptible to opportunistic infections that can be life-threatening.
Choice B Reason: Providing emotional support is an important aspect of providing care to this client, but it is not the highest priority, as it does not address the physical needs of the client.
Choice C Reason: Identifying risk factors related to contracting AIDS is not relevant for providing care to this client, as it does not help to improve the current condition or prevent complications.
Choice D Reason: Discussing the cause of AIDS is not essential for providing care to this client, as it does not affect the treatment or prognosis of the disease.
Correct Answer is D
Explanation
Choice A Reason: Calling the RN supervisor is not the priority action for the nurse, as it may delay the intervention and outcome.
Choice B Reason: Completing an incident report is not the priority action for the nurse, as it does not address the immediate problem or prevent further complications.
Choice C Reason: Checking the blood glucose level is not the priority action for the nurse, as it may confirm the error but not correct it.
Choice D Reason: Giving the client 15 to 20 g of carbohydrate is the priority action for the nurse, as it may prevent or treat hypoglycemia, which is a serious complication of insulin overdose.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today