A client presents with a possible bowel obstruction, and the nurse completes a detailed abdominal assessment. Which of the following clinical manifestations are consistent with a large bowel obstruction? (Select all that apply).
Profuse vomiting with fecal odor
Epigastric abdominal distention
Intermittent abdominal cramping
Ribbon-like stools or diarrhea
Metabolic acidosis
Severe fluid and electrolyte imbalance
Correct Answer : A,B,C,D,E,F
Choice A reason:Profuse vomiting with a fecal odor can occur in large bowel obstructions due to the backward flow of bowel contents.
Choice B reason:Epigastric abdominal distention is a common finding in bowel obstructions due to the accumulation of gas and fluids.
Choice C reason:Intermittent abdominal cramping results from the bowel's attempt to push contents through the obstructed area.
Choice D reason:Ribbon-like stools or diarrhea may occur if there is a partial obstruction allowing some contents to pass.
Choice E reason:Metabolic acidosis can develop due to the accumulation of lactic acid from tissue hypoxia and decreased perfusion.
Choice F reason:Severe fluid and electrolyte imbalance can result from vomiting and the inability to absorb fluids and nutrients properly.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
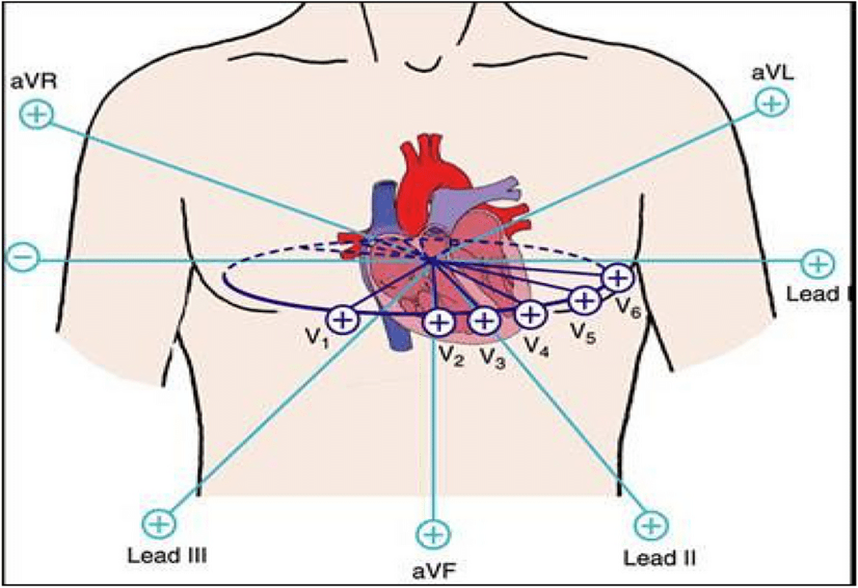
Choice A reason: A 12-lead ECG can reveal changes in the ST segment, T wave, and QRS complex, which are indicative of myocardial ischemia, injury, or infarction. It is the first line diagnostic test that needs to be recorded within 10 minutes after the first medical contact in cases of suspected acute coronary syndromes.
Choice B reason: While pain radiating to the left arm can be a symptom of MI, it is not a definitive diagnostic action. It is a common symptom but can also be associated with other conditions.
Choice C reason: Checking the client's blood pressure is important in the overall assessment of the client's cardiovascular status but does not specifically diagnose MI. Blood pressure can be normal, elevated, or decreased in the case of MI.
Choice D reason: Auscultating heart tones can provide information about the presence of murmurs, gallops, or rubs, but it is not a specific diagnostic action for MI. Heart sounds may be normal during an MI.
Correct Answer is ["35"]
Explanation
- Step 1: Identify the total volume to be administered. The nurse is scheduled to administer 840 mL of enteral nutrition over a 24-hour period.
- Step 2: Identify the total time over which the volume is to be administered. The total time is 24 hours.
- Step 3: Calculate the rate at which the infusion pump should be set. We can do this by dividing the total volume by the total time:
- Rate = Total Volume ÷ Total Time.
- Rate = 840 mL ÷ 24 hours.
- Calculating the division gives us: Rate = 35 mL/hr.
set the infusion pump to deliver 35 mL/hr.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today