A client is reporting pain in her casted leg. The nurse has administered analgesics and elevated the limb. Thirty minutes after administering the analgesics. the client states the pain is unrelieved. The nurse is unable to palpate the client's dorsalis pedis or posterior tibial pulse and the client's foot is pale. The nurse suspects compartment syndrome. What is the nurse's most appropriate action?
Promptly inform the primary provider.
Reassess the client's neurovascular status in 15 minutes.
Warm the client's foot and determine whether circulation improves.
Reposition the client with the affected foot dependent.
The Correct Answer is A
Explanation:
A. Promptly inform the primary provider:
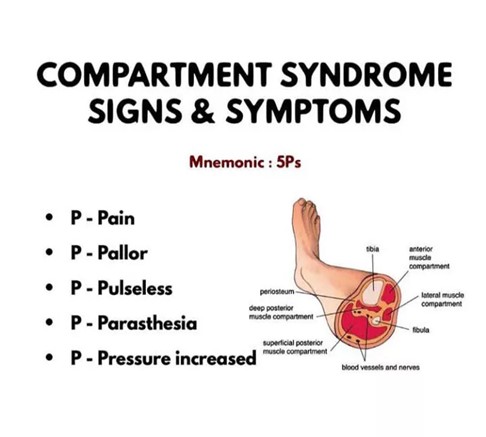
Explanation: Compartment syndrome is a medical emergency that requires immediate intervention. If a nurse suspects compartment syndrome due to symptoms like severe unrelieved pain, absent pulses, and pale extremities, the most appropriate action is to promptly inform the primary healthcare provider. The provider can assess the situation, order necessary diagnostic tests, and potentially arrange for emergent interventions like fasciotomy to relieve compartment pressure.
B. Reassess the client's neurovascular status in 15 minutes:
Explanation: Waiting for 15 minutes to reassess the client's neurovascular status is not appropriate in this situation. Compartment syndrome can progress rapidly, leading to irreversible tissue damage within a short time frame. Delaying assessment and intervention can result in significant complications.
C. Warm the client's foot and determine whether circulation improves:
Explanation: Warming the foot is not appropriate in this context. Compartment syndrome is caused by increased pressure within the muscle compartment, leading to compromised circulation. Warming the foot will not address the underlying issue of elevated compartment pressure and can potentially worsen the condition by dilating blood vessels and increasing pressure further.
D. Reposition the client with the affected foot dependent:
Explanation: Repositioning the client with the affected foot dependent is contraindicated in compartment syndrome. Elevating the limb can worsen the condition by further restricting blood flow. The limb should be kept at or slightly below the level of the heart to maintain adequate perfusion until medical intervention can be initiated.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["B","C","D","E"]
Explanation
A. Malunion: Malunion happens when a fractured bone heals in an improper position, leading to deformity and functional impairment. While it is a concern, it typically develops over time during the healing process and is not an immediate early complication that the nurse would monitor for in the acute phase following a fracture.
B. Compartment syndrome: Compartment syndrome is a serious condition that can occur after an injury, such as a fracture. When there is increased pressure within a muscle compartment, it can lead to reduced blood flow, potentially causing tissue damage and nerve injury. Prompt recognition and intervention are crucial to prevent complications.
C. Fat embolism: Fat embolism occurs when fat particles from the bone marrow or other sources enter the bloodstream, often after a long bone fracture or major trauma. These particles can travel to the lungs and other organs, causing respiratory distress, confusion, and other symptoms. Fat embolism is a significant concern in orthopedic trauma patients and requires careful monitoring.
D. Deep vein thrombosis (DVT): DVT is the formation of blood clots in deep veins, usually in the legs. Patients with fractures, especially those immobilized for extended periods, are at increased risk for DVT. If a clot dislodges and travels to the lungs, it can cause a pulmonary embolism, which is a life-threatening complication.
E. Pulmonary emboli: Pulmonary emboli occur when blood clots, often originating from DVT, travel to the lungs and block pulmonary arteries. This condition can lead to sudden difficulty breathing, chest pain, and even cardiac arrest. Pulmonary embolism is a medical emergency and requires immediate intervention.
Correct Answer is B
Explanation
A. Morse Scale:
The Morse Scale, also known as the Morse Fall Scale, is used to assess a patient's risk of falling. It evaluates various factors such as history of falling, secondary diagnosis, ambulatory aids, IV therapy, gait, and mental status. It is primarily focused on assessing the risk of falls, not pressure ulcers.
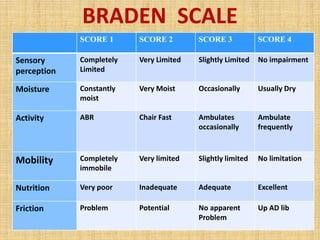
B. Braden Scale:
As previously mentioned, the Braden Scale assesses a patient's risk for developing pressure ulcers. It takes into account sensory perception, moisture, activity, mobility, nutrition, and friction/shear. The scale helps healthcare providers determine the level of risk a patient has for developing pressure sores and guides interventions to prevent them.
C. Bristol Scale:
The Bristol Stool Scale is used to classify the form of human feces into seven categories. It is a medical aid designed to classify the form of human feces into seven categories. This scale is primarily used to assess bowel movements and is unrelated to pressure ulcers.
D. Hendrich II Scale:
The Hendrich II Fall Risk Model is a tool designed to identify patients at risk for falls. It includes factors such as confusion, symptomatic depression, altered elimination, dizziness, male gender, and the use of antiepileptics, benzodiazepines, or non-opioid analgesics. Similar to the Morse Scale, it focuses on assessing the risk of falls, not pressure ulcers.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today