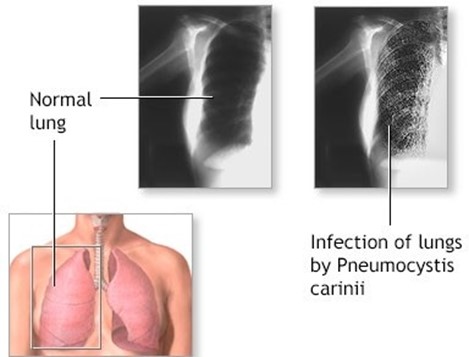
A client is hospitalized with Pneumocystis carinii pneumonia. The nurse notes that the client has had no visitors, seems withdrawn, avoids eye contact and refuses to take part in conversation. In a loud, angry voice the client demands that the nurse leave the room. The nurse formulates a diagnosis of Social isolation. Based on this diagnosis, what is an appropriate goal of care for the client? Select one answer
Identifying one way to increase social interaction
Returning a demonstration of measures that can increase independence
Identifying at least one factor contributing to altered sexuality paterns
Reporting increased adaptation to changes in health status
The Correct Answer is D
Choice A reason: Symptoms are subjective data that are reported by the client, such as pain, nausea, or fatigue. They are not observable or measurable by the nurse, and they may vary depending on the client’s perception or expression. The data that the PN discovered are not symptoms, but objective data that are observed or measured by the nurse, such as skin condition, oral mucus membranes, and temperature. Therefore, this choice is incorrect.
Choice B reason: Urinary retention is a condition in which the client is unable to empty the bladder completely or at all. It can cause symptoms such as difficulty or pain in urinating, frequent or urgent urination, or abdominal distension. It can also lead to complications such as infection, kidney damage, or bladder rupture. The data that the PN discovered are not related to urinary retention, but to dehydration or fever. Therefore, this choice is incorrect.
Choice C reason: Signs of fluid overload are objective data that indicate excess fluid in the body, such as edema, weight gain, crackles in the lungs, or elevated blood pressure. They can result from conditions such as heart failure,
kidney failure, or liver cirrhosis. The data that the PN discovered are not signs of fluid overload, but signs of fluid deficit or heat stroke. Therefore, this choice is incorrect.
Choice D reason: Data clustering is a process of grouping related data together to form a meaningful patern that can support a nursing diagnosis. It can help the nurse to identify the client’s problems, needs, or risks, and to prioritize and plan interventions accordingly. The data that the PN discovered are an example of data clustering, as they represent a patern of signs that indicate a possible problem such as dehydration or fever. Therefore, this choice is correct.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D"]
Explanation
Choice A reason: The nursing assistant is speaking in a normal tone is an action that the PN should not intervene in during communication with the client who is hearing impaired. Speaking in a normal tone can help the client to hear the natural variations and inflections of the voice, and to avoid distortion or confusion. Speaking in a high-pitched or
low-pitched tone can make the voice harder to hear or understand, especially if the client has a hearing loss in a specific frequency range. Therefore, this choice is correct.
Choice B reason: The nursing assistant is facing the client while speaking is an action that the PN should not intervene in during communication with the client who is hearing impaired. Facing the client while speaking can help the client to see the facial expressions and lip movements of the speaker, and to enhance visual cues and feedback. Facing away from the client while speaking can make the voice muffled or unclear, and can interfere with eye contact or rapport. Therefore, this choice is correct.
Choice C reason: The nursing assistant is speaking directly into the impaired ear is an action that the PN should intervene in during communication with the client who is hearing impaired. Speaking directly into the impaired ear can create an uncomfortable or unnatural position for the client and the speaker, and interfere with eye contact or facial expressions. Speaking directly into the impaired ear can also create a loud or distorted sound that may be unpleasant or painful for the client. Speaking face-to-face, and slightly toward the unaffected ear, can improve communication with a client who is hearing impaired. Therefore, this choice is incorrect.
Choice D reason: The nursing assistant is speaking clearly to the client is an action that the PN should not intervene in during communication with the client who is hearing impaired. Speaking clearly to the client can help the client to hear and understand the words and sentences of the speaker, and to avoid miscommunication or misunderstanding. Speaking unclearly to the client can make the voice garbled or incomprehensible, and can cause frustration or confusion. Therefore, this choice is correct.
Correct Answer is A
Explanation
Choice A reason: This is incorrect because it shows that the nurse is not using a systematic and evidence-based approach to care. The nurse’s notes are a form of documentation, not a source of planning.
Choice B reason: This is correct because it shows that the nurse is using a systematic and evidence-based approach to care. The nursing diagnosis is a clinical judgment that identifies the client’s actual or potential health problems or needs and provides the basis for selecting appropriate interventions.
Choice C reason: This is incorrect because it shows that the nurse is not using a holistic and individualized approach to care. The doctor’s orders are a form of prescription, not a source of planning.
Choice D reason: This is incorrect because it shows that the nurse is confusing the outcome with the process. The care plan is a written document that outlines the goals, interventions, and evaluation of care, not a source of planning.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today