A client is diagnosed with gestational hypertension and is receiving magnesium sulfate. Which finding would the nurse interpret as indicating a therapeutic level of medication?
Difficulty in arousing
Deep tendon reflexes 2+
Urinary output of 30 mL per hour
Respiratory rate of 10 breaths/minute
The Correct Answer is B
Choice A Reason: This is incorrect because difficulty in arousing is a sign of magnesium toxicity, which is a serious complication of magnesium sulfate therapy. Magnesium toxicity can cause central nervous system depression, muscle weakness, and cardiac arrest. The nurse should monitor the client's level of consciousness and stop the infusion if the client becomes lethargic or unresponsive.
Choice B Reason: This is correct because deep tendon reflexes 2+ indicate a normal and expected response to magnesium sulfate therapy. Magnesium sulfate is a muscle relaxant that can reduce the risk of seizures in gestational hypertension. The nurse should assess the client's deep tendon reflexes regularly and maintain them at 2+ or slightly diminished.
Choice C Reason: This is incorrect because urinary output of 30 mL per hour is below the normal range of 40 to 80 mL per hour and may indicate renal impairment or dehydration. Magnesium sulfate can cause renal toxicity or fluid retention, which can affect the urinary output. The nurse should monitor the client's urinary output and fluid balance and report any abnormalities to the doctor.
Choice D Reason: This is incorrect because respiratory rate of 10 breaths/minute is below the normal range of 12 to 20 breaths/minute and may indicate respiratory depression. Magnesium sulfate can cause respiratory depression or failure, which can be life-threatening. The nurse should monitor the client's respiratory rate and oxygen saturation and administer oxygen or antidote if needed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
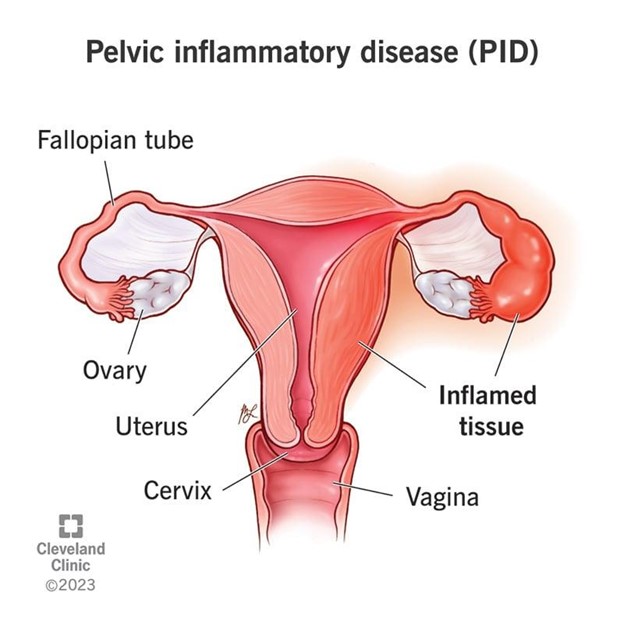
Choice A Reason: This is correct because recurrent pelvic infections, such as pelvic inflammatory disease (PID), can cause scarring and inflammation of the fallopian tubes, which can impair the normal movement of the fertilized egg to the uterus. This can increase the risk of ectopic pregnancy, which is a life-threatening condition where the fertilized egg implants outside the uterine cavity, usually in the fallopian tube.
Choice B Reason: This is incorrect because ovarian cysts are fluid-filled sacs that develop in or on the ovaries. They are usually benign and do not affect fertility or pregnancy. However, some types of ovarian cysts, such as endometriomas or dermoid cysts, may require surgery to remove them, which can cause damage to the ovaries or fallopian tubes and increase the risk of ectopic pregnancy.
Choice C Reason: This is incorrect because use of oral contraceptives for 8 years is not a risk factor for ectopic pregnancy. In fact, oral contraceptives can reduce the risk of ectopic pregnancy by preventing ovulation and fertilization. However, if a woman becomes pregnant while taking oral contraceptives, she should stop taking them and consult her doctor, as they may have adverse effects on the developing fetus.
Choice D Reason: This is incorrect because heavy, irregular periods are not a risk factor for ectopic pregnancy. They may indicate other conditions such as hormonal imbalance, uterine fibroids, polycystic ovary syndrome (PCOS), or endometriosis, which can affect fertility or pregnancy, but not necessarily cause ectopic pregnancy.
Correct Answer is C
Explanation
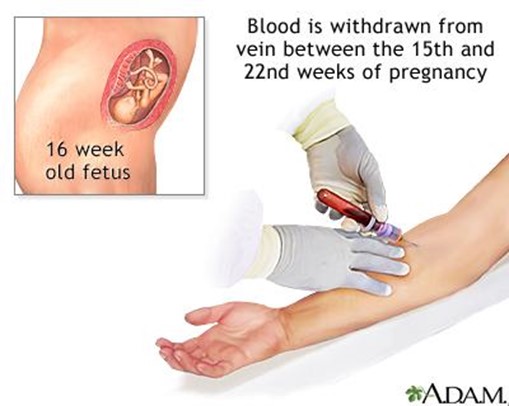
Choice A Reason: This is incorrect because sickle-cell anemia is a genetic disorder that affects the shape and function of red blood cells. It does not affect the AFP level, which is a protein produced by the fetus and placenta. Sickle-cell anemia can be detected by other prenatal tests, such as hemoglobin electrophoresis or DNA analysis.
Choice B Reason: This is incorrect because cardiac defects are structural abnormalities of the heart or blood vessels that affect the blood flow and oxygen delivery to the fetus. They may cause an increased AFP level, not a decreased one, as they can lead to fetal distress or edema. Cardiac defects can be detected by other prenatal tests, such as fetal echocardiography or ultrasound.
Choice C Reason: This is correct because Down syndrome is a chromosomal disorder that results from an extra copy of chromosome 21. It causes various physical and mental developmental delays and defects in the fetus. It is associated with a decreased AFP level, as well as decreased levels of human chorionic gonadotropin (hCG) and unconjugated estriol (uE3). Down syndrome can be confirmed by other prenatal tests, such as amniocentesis or chorionic villus sampling (CVS).
Choice D Reason: This is incorrect because respiratory disorders are problems that affect the breathing and gas exchange of the fetus. They may cause an increased AFP level, not a decreased one, as they can lead to fetal distress or edema. Respiratory disorders can be detected by other prenatal tests, such as fetal biophysical profile (BPP) or nonstress test (NST).
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today