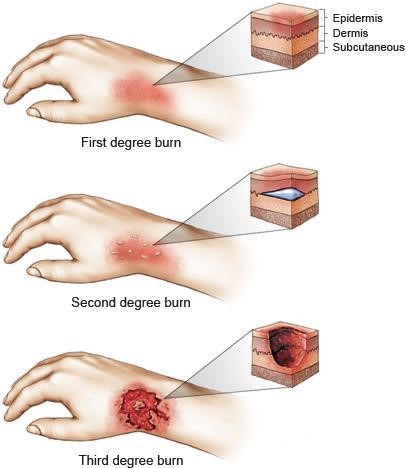
A client is brought to the emergency department with partial-thickness burns to his face, neck, arms, and chest after trying to put out a car fire. The nurse should implement which nursing actions for this client? (Select all that apply.)
Submerge client in a cold bath
Administer oxygen
Restrict fluids
Provide a meal high in fiber
Assess airway
Apply ice to burned areas
Correct Answer : B,E,F
Choice A Reason: This is incorrect because submerging the client in a cold bath can cause hypothermia, shock, or infection. Cold water can lower the body temperature and blood pressure, which can impair circulation and organ function. Cold water can also introduce bacteria or contaminants into the open wounds. The nurse should use cool water or saline to gently irrigate the burned areas and then cover them with sterile dressings.
Choice B Reason: This is correct because administering oxygen can help the client breathe better and prevent hypoxia. Burns to the face, neck, or chest can cause swelling or damage to the airway, which can impair gas exchange and oxygen delivery. Oxygen can also reduce the risk of carbon monoxide poisoning, which can occur from inhaling smoke or fumes.
Choice C Reason: This is incorrect because restricting fluids can worsen dehydration and shock. Burns can cause significant fluid and electrolyte loss through evaporation and leakage from damaged capillaries. This can lead to hypovolemia, which is low blood volume, and hypotension, which is low blood pressure. The nurse should monitor the client's vital signs, urine output, and weight, and administer intravenous fluids as ordered.
Choice D Reason: This is incorrect because providing a meal high in fiber can cause abdominal discomfort or diarrhea. Burns can cause paralytic ileus, which is a temporary loss of bowel function due to nerve damage or inflammation. This can impair digestion and absorption of food and cause nausea, vomiting, or constipation. The nurse should assess the client's bowel sounds and provide enteral or parenteral nutrition as ordered.
Choice E Reason: This is correct because assessing airway is a priority nursing action for a client with burns. As mentioned above, burns to the face, neck, or chest can compromise the airway and cause respiratory distress or failure. The nurse should assess the client's level of consciousness, breathing rate and pattern, oxygen saturation, and signs of inhalation injury, such as sooty sputum, singed nasal hairs, or hoarseness. The nurse should also be prepared to assist with intubation or tracheostomy if needed.
Choice F Reason: This is correct because applying ice to burned areas can help reduce pain and swelling. Ice can constrict blood vessels and numb nerve endings, which can decrease inflammation and sensation. However, ice should be applied for no more than 15 minutes at a time and wrapped in a cloth or towel to prevent frostbite or tissue damage. Ice should not be applied to large or deep burns.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
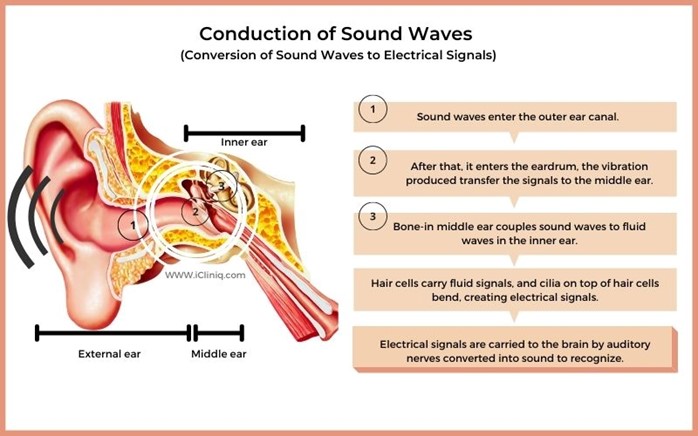
Choice A reason: This is incorrect because using sign language when communicating with the client is not an appropriate action for the nurse to take. Sign language is a form of communication that uses hand gestures, facial expressions, and body movements. It is not a universal language and requires training and practice. The nurse should not assume that the client knows or prefers sign language unless they have indicated so.
Choice B reason: This is incorrect because speaking loudly and into the client's good ear is not an appropriate action for the nurse to take. Speaking loudly can distort the sound quality and cause discomfort or irritation to the client. Speaking into the client's good ear can also create a sense of imbalance and isolation. The nurse should speak at a normal volume and tone, and face the client directly.
Choice C reason: This is the correct answer because speaking directly to the client in a normal, clear voice is an appropriate action for the nurse to take. Speaking directly to the client can help them see the nurse's mouth movements and facial expressions, which can enhance understanding and communication. Speaking in a normal, clear voice can help convey the message clearly and respectfully.
Choice D reason: This is incorrect because sitting by the client's side and speaking very slowly is not an appropriate action for the nurse to take. Sitting by the client's side can make it difficult for them to see the nurse's face and hear their voice. Speaking very slowly can also make the message unclear and patronizing. The nurse should sit in front of the client and speak at a normal pace.
Correct Answer is B
Explanation
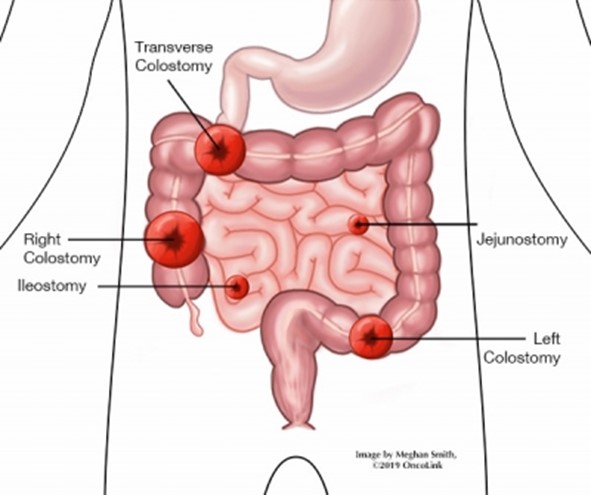
Choice A Reason: Soft pasty stool is normal for a transverse colostomy, as the stool has not reached the sigmoid colon where most of the water is absorbed.
Choice B Reason: This is the correct answer because purple discoloration of the stoma indicates ischemia or necrosis, which can lead to infection, perforation, or sepsis. It requires urgent intervention.
Choice C Reason: Stoma is beefy red is a normal finding for a healthy stoma, as it indicates adequate blood supply and healing.
Choice D Reason: There is skin excoriation around the stoma is a common complication of a colostomy, as the stool can irritate the skin. It can be managed with proper skin care and appliance fitting.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today